
Series Title: Structure-Function
A couple of friendly reminders:
- This is not medical advice. The content of this Newsletter is informational only.
- working memory <-- Yellow highlighted text are helpful links for you to click on.
- Member only content is at the bottom of the newsletter where you will receive...
- relevent links to resources and/or printables from the BOT Google Drive. If you are a member and have not been added to the drive for content, please request access by clicking this link.
- To go directly to the brand new structure-function folder in the BOT Google Drive for this series, click this structure-function link.
- Clinical conversation starters that take you a bit deeper than the documentation tips in this newsletter.
- If you want to learn more about the Functional Cognition Lab inside the BOT Portal, click here.
Picture This:

She has been coming to your outpatient clinic for three weeks. Early Alzheimer's diagnosis. Her daughter brings her because she can no longer drive safely.
The daughter reports that her mother gets lost. Not in unfamiliar places. In her own neighborhood. The street she has lived on for thirty-one years. She walks to the corner store she has visited hundreds of times and cannot find her way back.
Your team has documented disorientation, unsafe community mobility, and impaired short-term memory. The plan includes caregiver education, home safety assessment, and memory compensation strategies.
Nobody has asked why she cannot find her way back from the corner store.
They have asked what strategy she is missing and what compensatory tool she needs....but not, Why. Neurologically. What system is failing and what that system does.
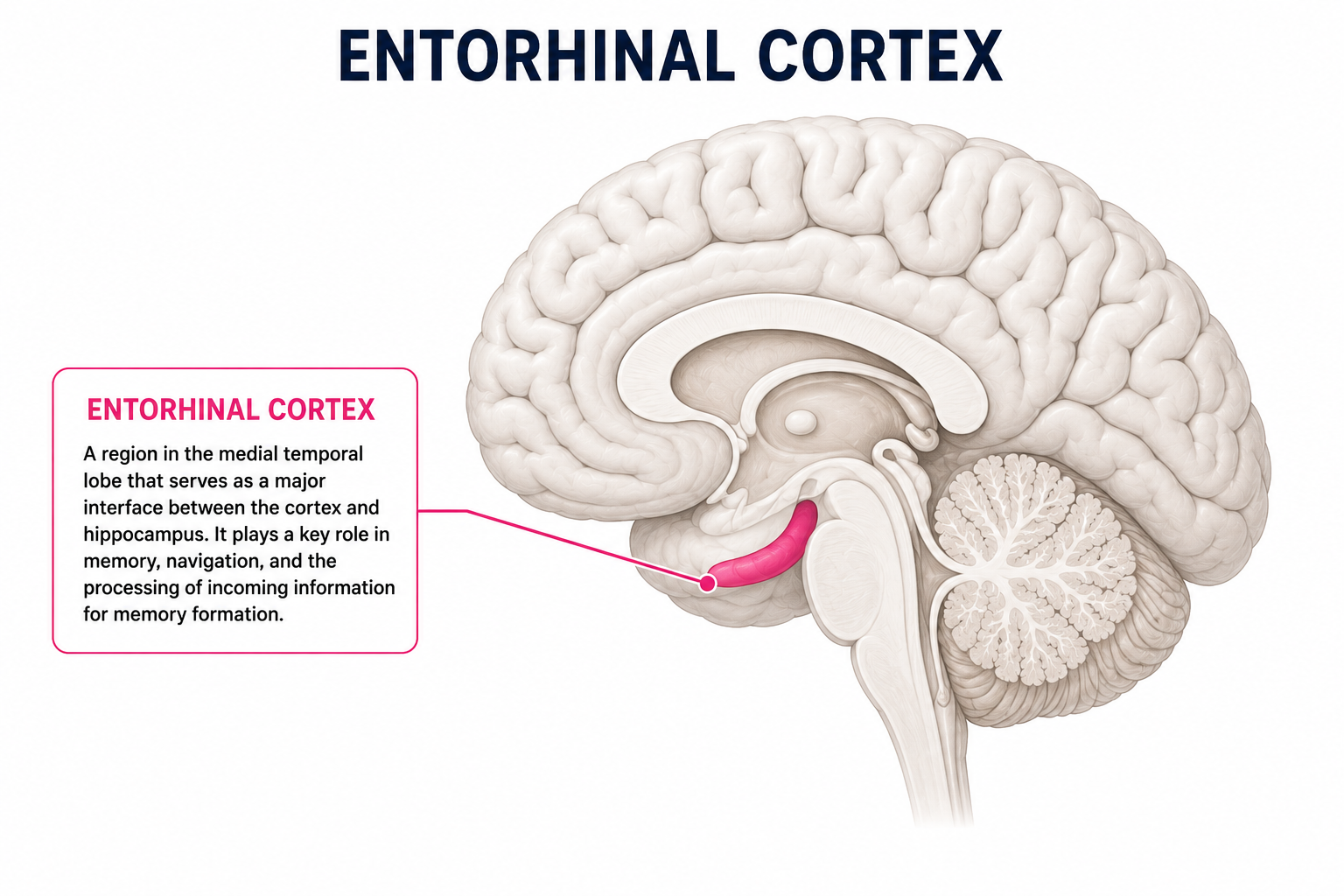
The entorhinal cortex is the earliest site of neurodegeneration in Alzheimer's disease. Its volume loss precedes hippocampal atrophy. It is where the brain builds and maintains its internal GPS (aka the spatial coordinate system that tells you where you are, where you have been, and how to get back).
>>>>When it degenerates, your patient does not lose a memory. They lose the system that converts spatial experience into a navigable map.
That is not a compensation problem.
That is a system failure.
And until you name it, your intervention will keep targeting the wrong thing.
Now, Picture This:
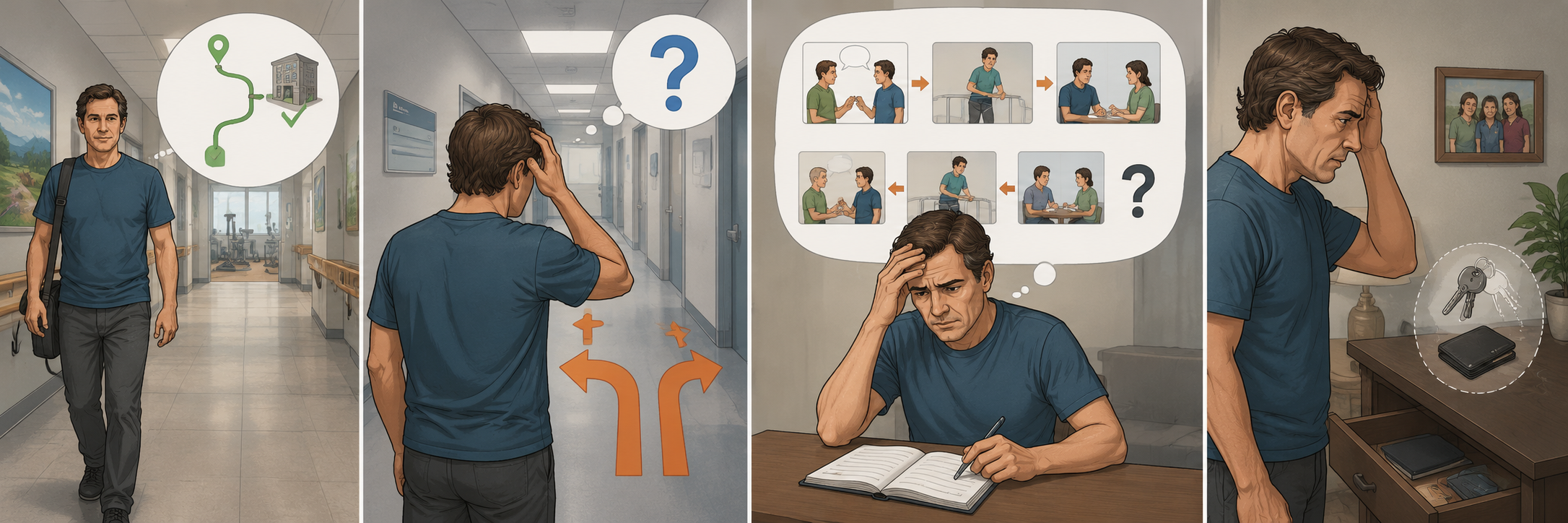
He is forty-four years old. Moderate TBI from a motor vehicle accident eight months ago. He has completed acute inpatient rehabilitation and is now in outpatient cognitive rehab.
He cannot learn new routes. He can walk to the therapy gym independently because he has been doing it for six weeks. Ask him to find a new room and he is lost within two turns. He cannot remember the sequence of events from earlier the same day. He describes conversations he had as though they happened in a different order than they did. He misplaces objects constantly because he cannot reconstruct the spatial and contextual memory of the moment he put them there, not because he forgets where he put them.
Your team has documented impaired short-term memory and attention deficits. The plan includes memory notebook training and attention remediation.
His entorhinal cortex has been compromised by diffuse axonal injury and neuroinflammation. The system that binds objects to their locations, events to their contexts, and experiences into coherent episodic memories is disrupted. A memory notebook does not rebuild that system. It compensates around it.
What is actually happening:
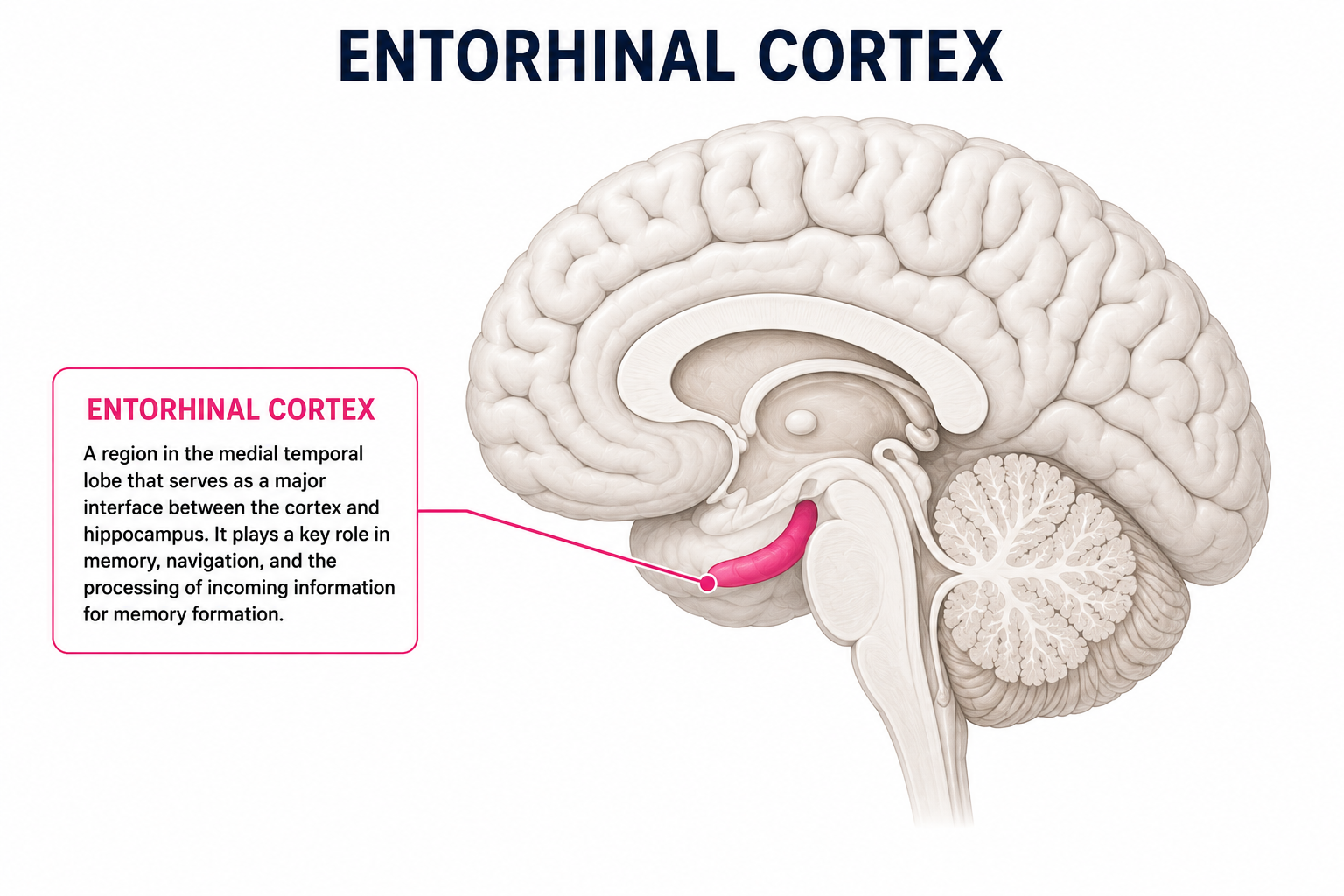
The entorhinal cortex is located in the medial temporal lobe at the front (rostral) portion of the parahippocampal gyrus. It sits between the neocortex, which processes information from our senses, and the hippocampus, which is responsible for forming new memories. Because of this location, the entorhinal cortex serves as the brain's primary gateway between perception and memory. It takes information about what you are currently seeing, hearing, and experiencing and organizes it so the hippocampus can store it as a lasting memory.
The entorhinal cortex carries out this role through two major information pathways.
- The anterior-lateral entorhinal cortex is primarily involved in recognizing what something is, such as identifying an object or a familiar face.
- The posterior-medial entorhinal cortex processes where something is located and the surrounding context, including where an event occurred and its relationship to the environment
- These two streams of information come together in the hippocampus, allowing the brain to combine an object with its location and context to form a complete episodic memory.
One of the entorhinal cortex's most important functions is supporting spatial navigation. This ability depends largely on specialized neurons called grid cells, which are found primarily in the medial entorhinal cortex. As we move through our environment, these cells create an internal map that helps us understand where we are and where we are going. Unlike landmarks that must be seen directly, this internal map allows us to maintain our sense of direction even as we turn, move, or temporarily lose visual cues.
Research has shown that the entorhinal cortex generates much of this spatial map independently before sending the information to the hippocampus. As the environment changes, additional neurons update the map by incorporating new landmarks and obstacles, allowing us to navigate unfamiliar settings, plan new routes, and adjust our movements without having to relearn the entire environment.
Because the entorhinal cortex links perception with memory while also supporting spatial orientation, damage to this region often produces two hallmark clinical symptoms: difficulty forming new episodic memories and impaired navigation. Individuals may recognize familiar objects or people but struggle to remember recent experiences, become disoriented in previously familiar places, or have difficulty learning the layout of a new environment. These deficits are particularly important clinically because the entorhinal cortex is among the earliest brain regions affected in Alzheimer's disease, making problems with navigation and episodic memory some of the earliest symptoms observed.
Take Action
Four observable signs that the entorhinal cortex is the disrupted system
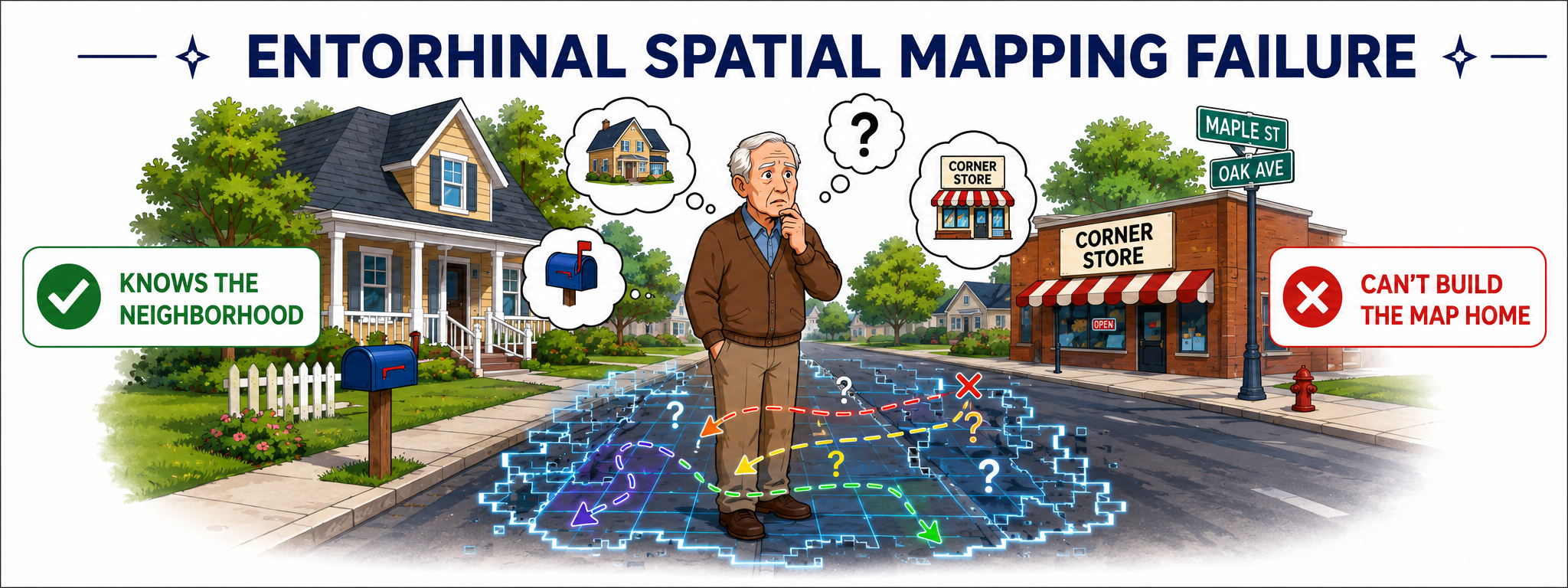
1. Getting lost in familiar places.
This is the cardinal entorhinal sign. The patient knows the neighborhood. They have walked the route hundreds of times. But they cannot reconstruct the spatial map that would guide them home. This is not confusion. It is grid cell system failure. The internal coordinate system that converts sensory experience into a navigable spatial map is not generating reliably.
If your patient is experiencing a disease that implicates the entorhinal cortex or medial temporal lobe, document it as navigational failure secondary to entorhinal spatial mapping disruption not as disorientation or unsafe community mobility. The only way we will be seen as the competetent professionals we are is if we use language that will show the world what we know...for a long time.
2. Failing to bind context to events.
The patient remembers that something happened but cannot recall where or when. They describe recent events out of sequence. They cannot reconstruct the contextual frame (aka the "what-where-when" binding) that makes an episodic memory retrievable as a experience. This reflects disruption of the entorhinal cortex's role in mediating the encoding and retrieval of associative recognition memory, specifically object-in-place and object-in-context tasks.
3. Misplacing objects without encoding their location.
The patient does not forget where they put something. They never encoded the spatial relationship between the object and its location in the first place. Object vector cells in the medial entorhinal cortex are responsible for encoding distance and direction from objects. When this system is disrupted, the patient cannot build the object-location binding that would make retrieval possible. A memory strategy does not fix this. It compensates around it.
4. New route learning fails despite intact procedural memory.
The patient can follow a familiar route automatically. They cannot learn a new one. Procedural memory for practiced routes is supported by the basal ganglia and is relatively preserved when the entorhinal cortex is disrupted. New spatial learning requires the entorhinal-hippocampal feedforward system to be intact. When it is not, the patient appears capable by moving well and following instructions, but novel routes do not consolidate (aka do get get stored into long term memory).
The setup:
Before you choose your intervention, probe the entorhinal system specifically in your session.
Ask the patient to describe the route from their front door to a familiar destination
- They do not need to speak from a memory of a map. Tell them to communicate the felt experience of walking it.
- Listen for whether they can generate a spatial sequence, whether landmarks appear in the correct order, and whether they can reconstruct turns and distances or only name the destination.
- Many people who are experiencing impairments will find this very challenging or express that it is silly or pointless. This is your opportunity to educate them on the importance of using this activity to exercise this part of the brain!
Ask them to tell you about something that happened yesterday.
- Listen not just for whether they remember it but for whether they can place it in context (like where they were, what came before it, what came after).
- Context binding is entorhinal. Isolated fact retrieval is not.
Give them a brief object placement task in your session space. Show them where three objects are placed, remove them from the room briefly, return, and ask them to replace the objects. This is an object-in-place task that directly probes entorhinal associative recognition memory.
These three probes take as little five minutes, but can be designed for an entire intervention module in your treatment! They tell you whether you are treating a memory system problem or a perception-to-memory interface problem. The intervention that follows is different depending on the answer.

How to Treat This (Real Sessions)
Spatial memory training grounded in entorhinal function:
- Because the entorhinal cortex generates spatial maps through active exploration and grid cell firing, passive review of routes does not train the system. Active navigation does.
- For patients where entorhinal function is partially intact and neuroplasticity is the goal, route learning needs to involve real spatial exploration (walking routes, returning to starting points, navigating to landmarks from multiple directions) not map review or verbal description.
- For patients where entorhinal degeneration is progressive, the goal shifts from rebuilding the system to maximizing the use of what remains. Consistent environments, predictable spatial layouts, and reduced environmental complexity reduce the demand on a failing grid cell system. Landmark-based navigation (using salient, emotionally significant landmarks rather than abstract spatial coordinates), can partially compensate for grid cell disruption by recruiting the lateral entorhinal object memory system instead.
Aerobic exercise and entorhinal volume:
- Aerobic fitness is positively correlated with entorhinal cortex volume in young subjects, indicating that regular aerobic exercise has structural effects on the medial temporal lobe memory system.
- This is the same neuroplasticity argument made for the hippocampus but with the entorhinal cortex as the primary target. For patients where entorhinal preservation is a clinical goal (early Alzheimer's, MCI, TBI recovery) aerobic exercise is a structural intervention, not a general health recommendation.
Sleep hygiene as entorhinal structural rehabilitation:
- Sleep is not a recovery variable. It is a structural rehabilitation requirement for the entorhinal cortex. A brief six-hour period of sleep deprivation following learning dramatically downscales the synaptic structures and density of specific interneurons in the entorhinal cortex, disrupting memory processing (Balendran et al., 2026).
- Sleep-dependent replay of neuronal firing patterns in the entorhinal cortex is essential for consolidating spatial and episodic memories. Without adequate sleep, the encoding that happened during waking hours does not consolidate.
- Every patient on your neurological caseload for whom memory consolidation is a treatment target needs sleep hygiene addressed explicitly and documented with this neurological rationale.
Across Disciplines
PT: Your patient's navigation failure in the community is not a safety and balance problem. It is an entorhinal grid cell system failure that is preventing new spatial map formation. Your gait and mobility training in novel environments like new hallways, new routes, new layouts is directly targeting the entorhinal spatial exploration system.Design your mobility sessions to include active route learning, landmark-based navigation, and return-to-origin tasks.
SLP: Your patient's difficulty with temporal sequencing of events, impaired new learning in functional communication contexts, and failure to bind conversational content to its context are entorhinal-hippocampal binding failures, not necessarily isolated memory or attention deficits. Your cognitive-communication interventions may target context encoding: where the conversation happened, what it followed, what it preceded. T
OT: Object-in-place failures like the patient not being able to find their glasses, cannot remember where they set down their medication, cannot reconstruct the spatial context of recent ADL performance are entorhinal object vector cell failures. Your intervention needs to reduce the spatial complexity of the environment while directly training consistent object-location associations. Compensation strategies that do not account for the encoding failure at the perception-to-memory interface will not generalize. Design your environment first. Train within it consistently. Then probe generalization deliberately.
Documentation
Identify and document:
- Entorhinal-specific deficit pattern: navigational failure in familiar environments, object-in-place binding failure, context-to-event binding impairment, new route learning failure with intact procedural memory
- System implicated: entorhinal cortex as the perception-to-memory interface; distinguish from hippocampal retrieval failure or prefrontal working memory disruption
- Probe results: route description task, context binding probe, object-in-place task; document what specifically failed and at what point in the task
- Intervention rationale: spatial exploration training, aerobic exercise as structural intervention, sleep hygiene as entorhinal consolidation requirement, dopaminergic session conditions, hemispheric lateralization of spatial training tasks
- Stimulation approach where applicable: temporal interference or deep brain stimulation target, hemisphere, and functional goal
Do not write: patient demonstrated impaired short-term memory and difficulty with orientation. Memory compensation strategies introduced.
Write what actually happened:
- Patient presents with early Alzheimer's disease with entorhinal cortex degeneration identified as the primary system disruption underlying observed navigational failure and episodic memory binding impairment.
- Entorhinal-specific probes administered: patient unable to generate spatial sequence for familiar route from home to corner store described three recent events without temporal or contextual binding. Could name events but not place them in sequence or location.
- Object-in-place task failed at three of three object locations with no self-detected errors. Findings consistent with grid cell system disruption and object vector cell failure rather than hippocampal retrieval deficit or prefrontal working memory impairment.
- Intervention plan targets active spatial exploration in consistent environments with landmark-based navigation training to recruit lateral entorhinal object memory system as compensatory pathway.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!

What's included:
[Resource 1] Home Activity Program - HAP targeting topigraphical orientation and naviagation. Simple to Complex Maps/Questions for your client to use in-session or between sessions.
[Resource 2] Dual Tasking Assessments and Interventions
Handout 1: Map Activities: Navigation, Inference, and Spatial Reasoning
This is your structured at-home cognitive activity resource for patients where entorhinal degeneration is progressive and the clinical goal has shifted from rebuilding spatial mapping capacity to maximizing the use of what remains. It includes three maps at progressively increasing cognitive demand, each with navigation questions, inferential questions, and for Map 3, a full scenario task requiring multi-step temporal planning and route adjustment under changing conditions.
Clinical tip: This resource is not a spatial exploration tool and should not be positioned as one. Active spatial exploration — walking routes, returning to starting points, navigating to landmarks from multiple directions — is what trains the entorhinal grid cell system when neuroplasticity is still the goal. These maps do not replicate that. What they do provide is a structured cognitive activity that exercises residual spatial reasoning, working memory, and inferential thinking in a safe, controlled format appropriate for patients who can no longer safely or reliably engage in active community navigation. Assign Map 1 Navigation as your in-session baseline probe before prescribing any map level as a home activity.
Spatial Memory Training Program Patient Guide - Active Entorhinal Training
Handout 2: Navigation Abilities Handout
This is your patient and family education resource for understanding the cognitive systems that support navigation and spatial orientation. It explains topographical organization, mental map formation, route planning, and spatial awareness in plain language, and connects those functions to the brain regions responsible — including the hippocampus, parietal lobe, and prefrontal cortex. Use it to help patients and families understand why navigational failure is a cognitive and neurological finding, not a safety or attention problem.
Clinical tip: Use the practical examples at the end of the handout — finding your way in a new city, navigating in the dark, driving with GPS — as your conversation anchor. Ask the patient or family which of those scenarios has become difficult. Their answer tells you exactly where the spatial memory system is breaking down and gives you your functional intervention target for the session.
One-Line Clinical Reasoning Starters
Navigational Failure — Entorhinal Grid Cell System Disruption
- Entorhinal cortex grid cell system disruption identified as the primary mechanism underlying navigational failure in familiar environments
- Patient unable to generate spatial sequence for practiced routes indicating internal coordinate system failure rather than procedural memory impairment
- Skilled spatial exploration training targeting active route learning and landmark-based navigation indicated to recruit lateral entorhinal object memory system as compensatory pathway.
Object-In-Place Binding Failure
- Entorhinal object vector cell failure identified as the mechanism underlying consistent object misplacement
- Patient unable to encode spatial relationship between objects and their locations despite intact attention and procedural memory
- Intervention targets consistent object-location association training within simplified spatial environment
- Compensation strategies alone are insufficient without addressing the perception-to-memory binding failure at the entorhinal interface.
Context-to-Event Binding Impairment — TBI
- Entorhinal-hippocampal binding disruption identified following moderate TBI
- Patient demonstrates event recall without contextual binding — can name events but cannot place them in spatial or temporal sequence
- Anterior-lateral and posterior-medial entorhinal systems implicated
- Skilled cognitive intervention targeting context encoding in functional communication and ADL contexts indicated
- Memory notebook training insufficient as primary intervention without addressing the interface failure upstream of hippocampal consolidation.
Sleep Hygiene as Entorhinal Structural Rehabilitation
- Sleep deprivation identified as active structural threat to entorhinal consolidation
- Patient reporting fragmented sleep
- Neurological rationale provided that sleep-dependent entorhinal replay is required for consolidation of spatial and episodic learning from each therapy session
- Sleep hygiene documented as entorhinal structural rehabilitation intervention, not lifestyle recommendation
- Referral placed for sleep evaluation
- Session learning targets will not consolidate without adequate sleep architecture.
Aerobic Exercise as Entorhinal Volume Intervention
- Aerobic exercise prescribed as structural intervention targeting entorhinal cortex volume preservation in patient with early Alzheimer's disease
- Evidence base supports positive correlation between aerobic fitness and entorhinal volume in the medial temporal lobe memory system
- Exercise documented as neuroplasticity intervention, not general health recommendation
- Session design includes pre-session aerobic bout as neuroplasticity primer and long-term aerobic program as entorhinal structural maintenance strategy.


Responses