Series Title: Structure-Function
A couple of friendly reminders:
- This is not medical advice. The content of this Newsletter is informational only.
- working memory <-- Yellow highlighted text are helpful links for you to click on.
- Member only content is at the bottom of the newsletter where you will receive...
- relevent links to resources and/or printables from the BOT Google Drive. If you are a member and have not been added to the drive for content, please request access by clicking this link.
- To go directly to the brand new structure-function folder in the BOT Google Drive for this series, click this structure-function link.
- Clinical conversation starters that take you a bit deeper than the documentation tips in this newsletter.
- If you want to learn more about the Functional Cognition Lab inside the BOT Portal, click here.
Picture This:
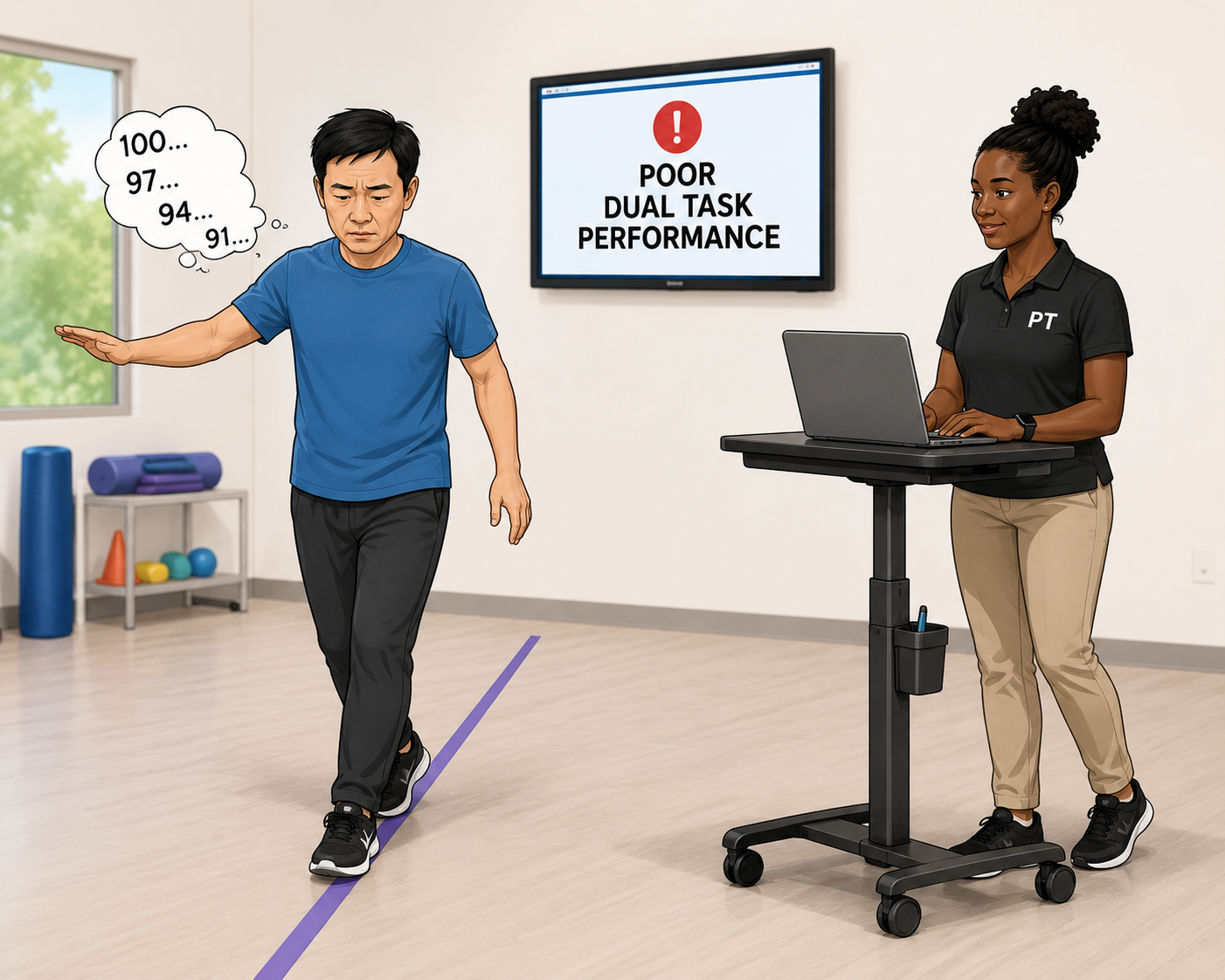
He has Parkinson's disease. He has been in PT for six weeks working on gait and balance. His therapist is good. She times him. She tracks his steps. She progresses him consistently.
Last week she added a dual task. Walk and count backward from 100 by threes. He immediately slowed down, lost his place in the count, and nearly lost his balance at the turn.
She documented poor dual task performance. She planned to increase the cognitive load next session.
She did not consider whether his prefrontal cortex had the capacity to handle the load she had already given him.
It did not.
In Parkinson's disease the prefrontal cortex is already operating near ceiling on single tasks. The dopaminergic depletion that drives motor symptoms simultaneously degrades the prefrontal resources that govern attention, working memory, and task coordination.
When a basic single task like walking already overtaxes the prefrontal network, adding a secondary cognitive demand does not train the system. It collapses it.
The patient slows, loses accuracy, and sometimes falls. Not because the task was too hard, but because the clinician did not know where the ceiling was before they pushed past it.
Now, Picture This:
She had a stroke four weeks ago. Left hemisphere. The imaging report said left CVA. The team said stroke protocol.
She sits in the therapy room and does not initiate. She needs a verbal cue to begin every task. She loses track of what she is doing mid-sequence. When the clinician gives multi-step instructions she can repeat the first step and nothing else.
The team has documented poor motivation, limited carry-over, and impaired short-term memory.
Nobody has looked at where the lesion is. Nobody has asked what the left dorsolateral prefrontal cortex does. Nobody has connected the initiation failure to the medial PFC, the working memory breakdown to the DLPFC, or the inability to hold a sequence to the disruption of the prefrontal-hippocampal network that organizes episodic memory and task context.
She is not unmotivated. She does not have a memory problem in the conventional sense.
She has a prefrontal network disruption that is presenting exactly the way prefrontal network disruption presents, and nobody on her team was ever taught to recognize it.
What is actually happening:
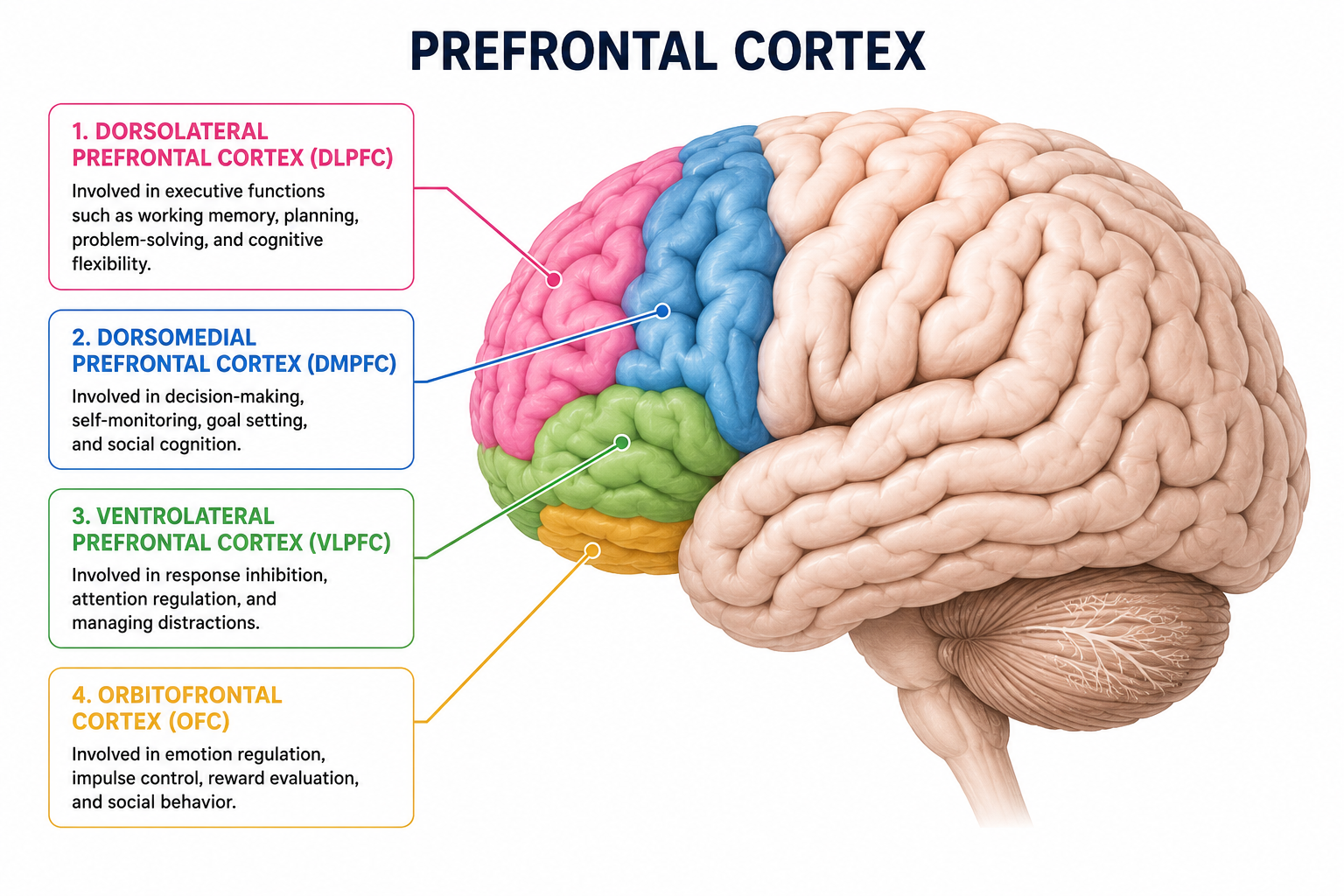
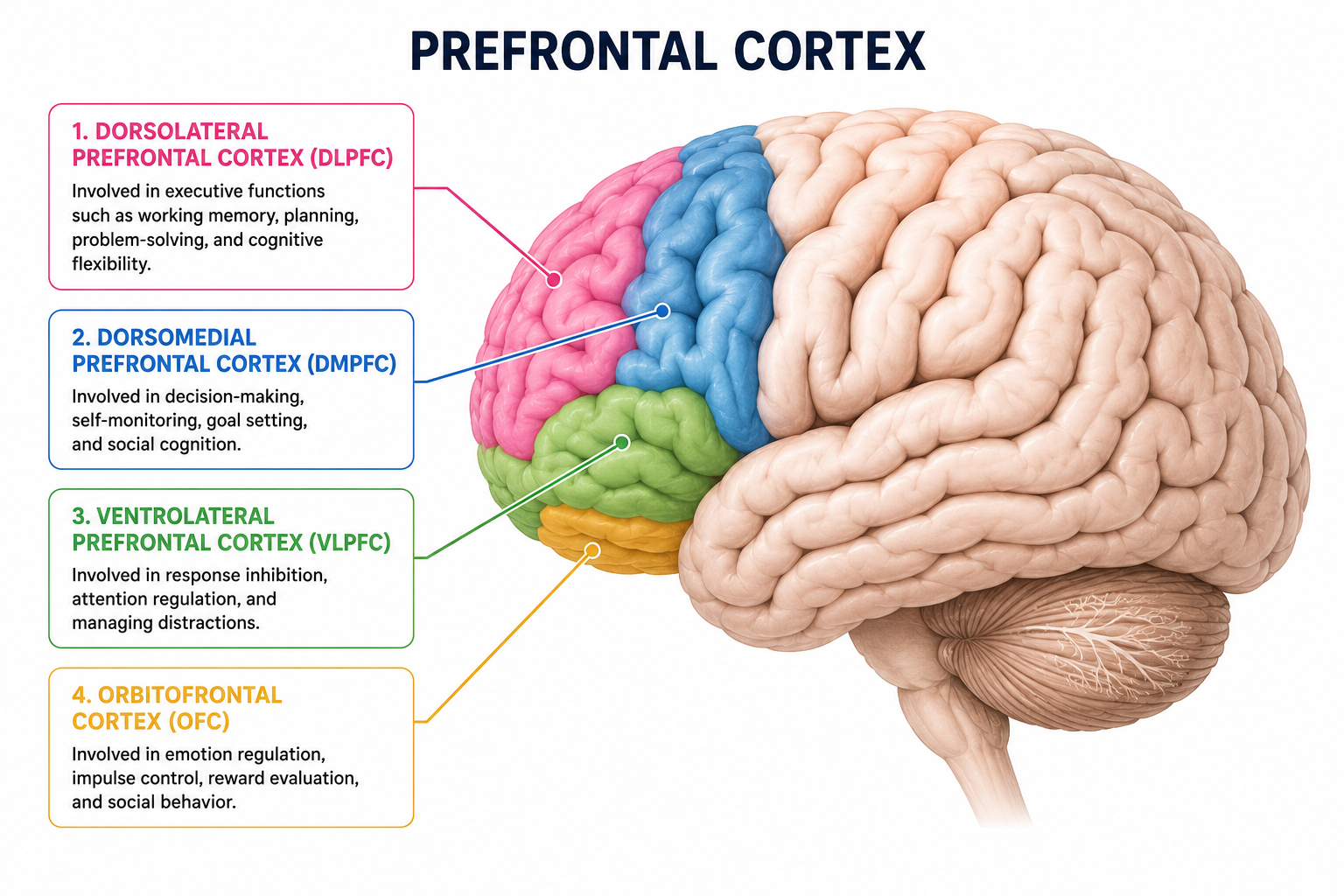
The prefrontal cortex is not a single structure. It is a collection of functionally distinct subregions that together make up the brain's executive command system, and almost nothing the brain does happens without its involvement.
The dorsolateral prefrontal cortex governs working memory, cognitive flexibility, planning, and the sequencing of goal-directed behavior. When it is disrupted, your patient cannot hold information across the steps of a task, cannot adapt when something changes, and cannot generate the internal sequence that turns intention into action.
The orbitofrontal cortex governs risk assessment, impulse control, emotional regulation, and decision-making. When it is disrupted, your patient makes poor choices, responds emotionally in ways that seem disproportionate, and cannot evaluate whether what they are doing is working.
The medial prefrontal cortex governs motivation, initiation, and social cognition When it is disrupted, your patient does not start — not because they are lazy or depressed, though mood compounds it — but because the internal go-signal that moves a person from intention to action is neurologically offline.
These subregions operate as a network, connecting downward to the supplementary motor area and primary motor cortex to execute movement laterally to the anterior cingulate cortex to monitor errors and allocate attention, and bidirectionally with the hippocampus to organize memory within context and across time.
During dual task walking specifically, lateral regions of the prefrontal cortex become associated with the attention-demanding cognitive aspects of the task, while medial regions primarily handle motor execution. Older adults and individuals with Parkinson's disease demonstrate an over-reliance on prefrontal resources during dual task walking as a compensatory mechanism to maintain performance despite reduced locomotor automaticity.
In Parkinson's disease this compensation reaches a ceiling. Single tasks already overtax available prefrontal resources, preventing proportional cortical activation when a secondary cognitive demand is added. A similar pattern has been observed in individuals with knee osteoarthritis, who rely heavily on top-down prefrontal control to maintain gait stability during both single and dual task walking to compensate for pain and reduced automaticity
Chronic stress adds another layer. Sustained elevation of cortisol triggers structural changes in the PFC including dendritic atrophy, reduced synaptic density, and decreased gray matter volume in the DLPFC specifically. This means a patient managing chronic pain, grief, social isolation, or the stress of a new diagnosis is not just emotionally compromised. Their prefrontal cortex is physically less capable of the cognitive work your intervention requires.
Take Action
Four signs the PFC is at or near ceiling before you add more demand.
1. Performance degrades when two things are required simultaneously.
The patient walks fine alone. They count fine sitting down. The moment you combine them, both collapse. In Parkinson's disease the prefrontal ceiling effect means that basic single tasks already consume available prefrontal resources, leaving nothing to allocate when a secondary cognitive demand is introduced. Do not increase load. Find the ceiling first.
2. Errors increase as the session progresses.
The patient performs reasonably at the start of the session and deteriorates over time without a physical explanation. Error rate is your proxy for prefrontal fatigue. When errors cluster in the second half of the session the PFC has depleted its available resources and can no longer monitor and correct performance. A significant positive correlation has been found between prefrontal activation and error count during cognitive-motor tasks, meaning error tracking can be used as a proxy for prefrontal load in clinical settings where neuroimaging is not available.
3. Initiation requires repeated external cueing.
The patient knows what to do. They have done it before. But they do not begin without being told. Every time. This is medial PFC dysfunction. The internal go-signal is not generating independently. Adding more verbal instruction does not fix it. Designing external structure into the environment does.
4. Perspective-based errors are disproportionate to physical capacity.
When you demonstrate a movement facing the patient (aka third person perspective) they make significantly more errors than when you stand beside them. Teaching cognitive-motor limb exercises using third person perspective, which requires mental rotation, activates the anterior half of the prefrontal cortex more effectively than first person perspective instruction. Error elevation under third person instruction is your noninvasive proxy for prefrontal activation load.
The setup:
Before you choose your dual task load, your instruction perspective, or your session complexity, establish the baseline.
Run the motor task alone. Time it. Note quality. Then add the cognitive element and measure the dual task cost. The difference between single task and dual task performance in both speed and accuracy. That cost is your PFC load index for this patient on this day.
If the cost is high, you will see significant slowing, accuracy collapse, or behavioral disorganization. This may mean the PFC is already near ceiling. You grade down, not up. You reduce the cognitive demand until performance stabilizes across two consecutive sessions before you advance.
If the patient is making errors under third person perspective instruction but performing cleanly under first person perspective, you have a grading lever that requires no equipment change. Perspective is your cognitive load dial. Turn it deliberately.
Document the baseline. Document the cost. Document the perspective condition. Every session. That data is your progression map and your justification for skilled care.

How to Treat This (Real Sessions)
Dual task grading for Parkinson's disease:
The ceiling effect is your primary clinical constraint . Begin with the motor task alone and establish a stable baseline before introducing any cognitive element. Targeted dual task training utilizing low to moderate cognitive loads is specifically recommended for Parkinson's disease patients, allowing them to practice neural resource reallocation without overtaxing their prefrontal networks. Document which cognitive load level produced stable dual task performance and advance only when the patient demonstrates consistent performance across two sessions at the current level.
Third person versus first person perspective dosing:
Third person perspective requires mental rotation and activates the anterior PFC more strongly than first person perspective, and produces significantly more errors at task onset which suggests that prefrontal demand is highest at initiation and the brain adapts as the session continues. Use third person when you want higher prefrontal engagement and the patient has available capacity. Use first person when you want to reduce cognitive load without changing the movement itself, or when errors under third person are demoralizing or functionally counterproductive. Error count under each perspective condition is your proxy for prefrontal activation .
tDCS targeting the DLPFC:
Anodal transcranial direct current stimulation targeting the dorsolateral prefrontal cortex can significantly enhance dual task gait performance, particularly walking speed, in patients with Parkinson's disease. The DLPFC is causally involved in voluntary task-order coordination, allowing individuals to intentionally schedule the processing sequence of overlapping tasks — and anodal tDCS applied to this region significantly reduces reaction times during intentional task switching. Where tDCS is available in your setting, DLPFC targeting is a supported adjunct to cognitive-motor training for this population.
Exercise as PFC primer:
Aerobic and resistance exercise interventions increase BDNF levels, promote neurogenesis, enhance synaptic plasticity, and increase overall PFC volume over time. Cognitive and motor dual task gait training promotes neuroplasticity by strengthening the activation and functional connectivity of the prefrontal cortex, subsequently improving attention, executive function, and balance in post-stroke patients . A brief aerobic bout before your cognitive or cognitive-motor intervention is neurological preparation. Name it that way in your documentation.
Virtual reality and artificial intelligence can be integrated with cognitive training programs to enhance patient engagement, motivation, and treatment effectiveness during stroke rehabilitation where these tools are available.
Sleep and stress as PFC recovery tools:
Sleep hygiene interventions improve sleep quality and directly enhance PFC function, aiding in recovery from stress-induced physiological changes. Mindfulness-based stress reduction and meditation practices increase gray matter density in the PFC and improve top-down regulation of stress responses. Anti-inflammatory approaches and interventions that modulate the cAMP-PKA-CREB signaling pathway can directly enhance neuroplasticity and mitigate neuroinflammation associated with chronic stress. These are not lifestyle suggestions. They are neuroplasticity interventions. Document them with that rationale.
Across Disciplines
PT: Your dual task gait training is a prefrontal intervention whether you have named it that way or not. The DLPFC coordinates the attention-demanding aspects of dual task walking while medial regions handle motor execution. When your Parkinson's patient fails the cognitive element during gait, that is a PFC ceiling finding, not a cognition referral. Dose it accordingly and document the neurological rationale.
SLP: Cognitive-communication tasks that require holding information, sequencing responses, and self-monitoring under conversation load are DLPFC tasks . When your patient loses their train of thought mid-sentence, repeats themselves without awareness, or cannot follow a multi-step instruction, you are watching prefrontal network disruption in real time. Your treatment targets the network. Name it.
OT: ADL sequencing, medication management, meal preparation, and any multi-step functional task require sustained DLPFC engagement for working memory, sequencing, and error monitoring. When your patient cannot complete a morning routine independently, ask which PFC subregion is implicated before you choose a compensatory strategy. The answer changes whether you design external structure, target initiation directly, or address working memory load specifically.
Across all disciplines: The perilesional inflammation that surrounds a subacute stroke lesion is not static. The network disruption it causes is most severe in the first weeks and can improve substantially with targeted input to the affected systems. This is your window. Precise, system-targeted intervention during the subacute phase capitalizes on neuroplasticity in a way that generic rehabilitation does not.
Know the region. Target the system. Document the network. Treat the window.
Documentation
Identify and document:
- PFC subregion implicated: DLPFC for working memory and sequencing, orbitofrontal for decision-making and impulse control, medial PFC for initiation and motivation; document which subregion's functions map onto the observed deficits
- Dual task cost: quantified difference between single task and dual task performance in speed and accuracy; documented as primary PFC load index
- Perspective condition: whether third person or first person instruction was used, error count under each condition, and clinical rationale for perspective selection
- Ceiling indicators: error clustering, performance degradation across session, initiation failure frequency, dual task cost percentage
- Neuroplasticity interventions: pre-session exercise bout, sleep hygiene referral, stress reduction referral; each documented with neurological rationale not lifestyle framing
Do not write: patient demonstrated difficulty with dual task activities and required frequent cueing to initiate tasks.
Write what actually happened:
- Patient presents with left hemisphere CVA with disruption to DLPFC-mediated working memory and medial PFC-mediated initiation networks. Initiation failure documented at all within-session task transitions internal go-signal not generating independently; external structure implemented to reduce initiation demand while initiation training progresses.
- Dual task assessment administered: single task tandem walk completed in 18 seconds with intact quality dual task cost measured at 34% speed reduction with two sequencing errors, indicating PFC load above available capacity at current cognitive demand level. Cognitive element reduced to low load for next session.
- Pre-session five-minute aerobic walk implemented as neuroplasticity primer prior to cognitive-motor training. Skilled intervention indicated to target PFC network disruption with precision-dosed dual task training and structured initiation protocol.
- Third person perspective instruction produced significantly higher error rate than first person across arm movement sequence, perspective condition documented as grading variable with first person instruction selected to maintain task quality while PFC capacity is rebuilt.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!

What's included:
[Resource 1] Acquired Brain Injury Symptoms (Major Brain Structures)
[Resource 2] Dual Tasking Assessments and Interventions