
A couple of friendly reminders:
- This is not medical advice. The content of this Newsletter is informational only.
- working memory <-- Yellow highlighted text are helpful links for you to click on.
- Member only content is at the bottom of the newsletter where you will receive...
- relevent links to resources and/or printables from the BOT Google Drive. If you are a member and have not been added to the drive for content, please request access by clicking this link.
- Clinical conversation starters that take you a bit deeper than the documentation tips in this newsletter.
- If you want to learn more about the Functional Cognition Lab inside the BOT Portal, click here.
Picture This:

Your patient comes in three times a week.
They do their exercises. They complete their tasks. They follow your instructions. On paper the session looks productive. You document participation. You document effort. You document compliance.
And then nothing carries over.
Not the home program. Not the strategy you practiced twelve times. Not the routine you built together over six weeks.
You add more repetitions. You simplify the task. You print another handout.
Nothing changes.
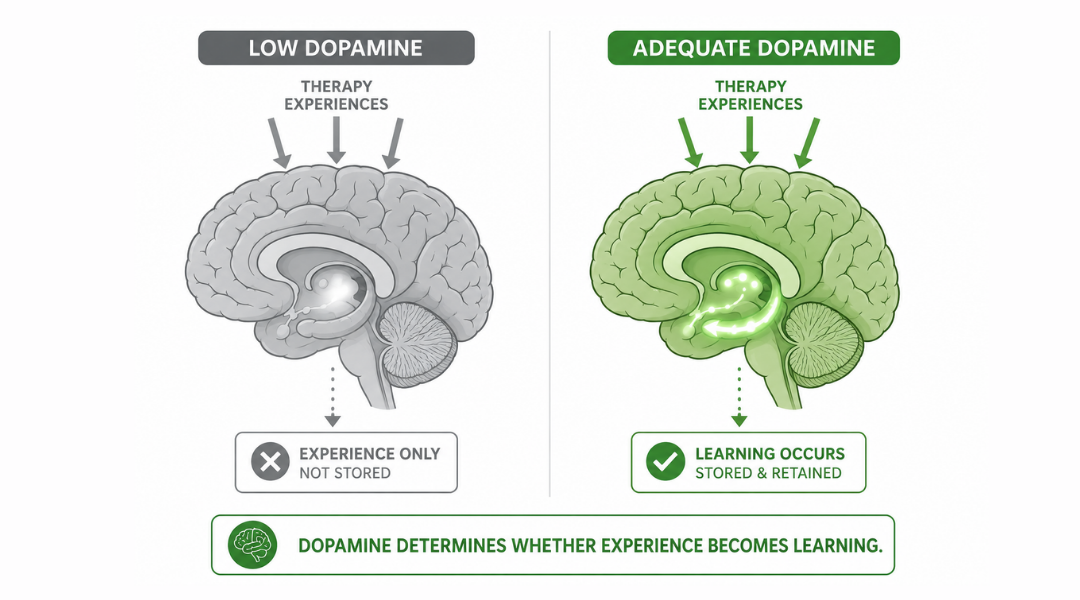
Here is what nobody told you in school: repetition without neurochemical readiness is not learning. It is rehearsal. And rehearsal without the right brain chemistry does not build new pathways. It fills time⏳.
The question is not how many times your patient practiced. The question is whether their brain was in a state to learn anything at all when they did.
That question has a neurological answer. And it starts with dopamine🔬.
What is actually happening:
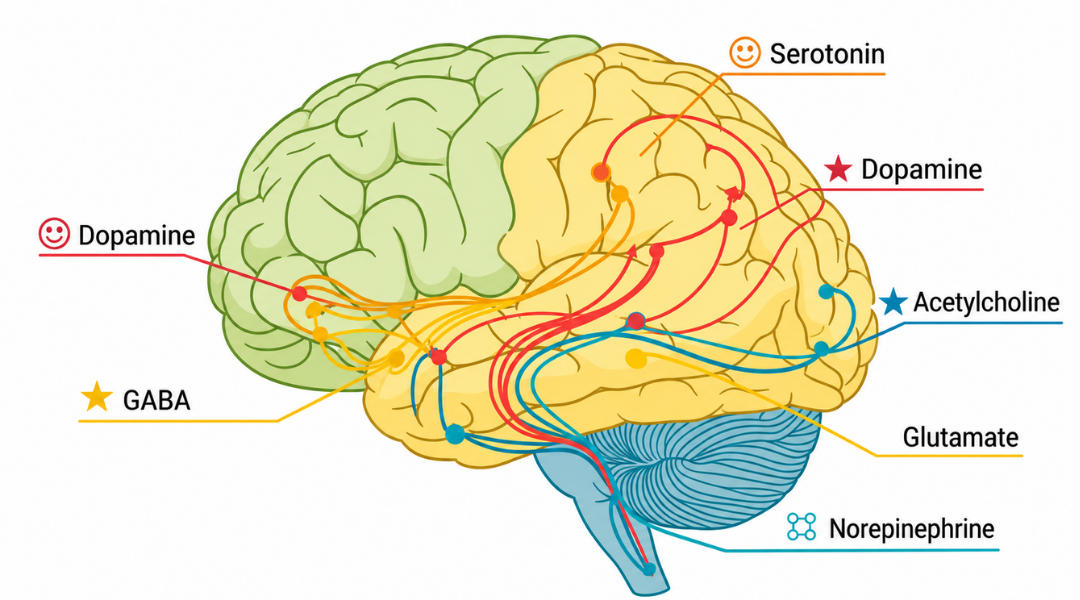
Dopamine is produced primarily in the substantia nigra and the ventral tegmental area and released into circuits throughout the brain (including the basal ganglia, the prefrontal cortex, and the hippocampus). It is not simply a mood chemical. It is the brain's signal for relevance, readiness, and reward.
When dopamine is available, the brain flags an experience as worth encoding.
- Attention sharpens.
- The basal ganglia consolidate the motor and behavioral patterns being practiced.
- The hippocampus begins building the memory trace.
- The prefrontal cortex stays online long enough to monitor and adapt.
When dopamine is low, none of that happens efficiently.
- The brain is present but not primed.
- Your patient is in the room but their neurochemistry is not ready to learn.
Low dopamine does not look dramatic. It looks like fatigue. It looks like slow initiation. It looks like a patient who tries but cannot seem to retain what you just worked on. It looks like the carry-over problem you have been calling motivation.
It is not motivation. It is neurochemistry. And the conditions that drive dopamine down in your patient population are almost universal: chronic illness, pain, social isolation, disrupted sleep, loss of meaningful role, and a rehabilitation schedule that prioritizes physical output over neurological readiness.
Every discipline is treating in these conditions every day. Almost no one is addressing them before the session begins.
Take Action
Before you begin your intervention, assess whether your patient's brain is in a state to learn from it.
This is not a formal assessment. It is three observations and one question.
Observe initiation. Does your patient engage willingly or do they require significant effort to begin? Low initiation is a dopamine signal. The basal ganglia are not generating enough drive to move from intention to action.
Observe affect. Is your patient flat, withdrawn, or going through the motions? Affect reflects the reward system's baseline state. A patient with flat affect is not unmotivated. Their reward circuitry is underactivated.
Observe carry-over from last session. Not just whether they practiced at home. I am talking about whether anything from last session is accessible right now. Dopamine-dependent learning consolidates during sleep and through meaningful repetition in context. If nothing carried over, the encoding conditions were insufficient.
Ask one question: What did you do yesterday that you enjoyed?
That question is not small talk. It is a clinical probe. A patient who cannot identify a single enjoyable activity from the previous day is a patient whose dopamine system has very little to work with. That finding changes your session before it starts.
The setup:
You are not a pharmacist. You cannot prescribe dopamine.
But you can design sessions and recommend lifestyle conditions that support the neurochemical environment your intervention requires.
This is what that looks like in practice.
Meaningful activity is not a philosophy. It is a dopamine delivery mechanism. When a patient engages in something personally relevant (that is, something connected to their identity, their roles, their relationships, their history), the brain releases dopamine in anticipation and in response. That release primes the learning system. Your intervention lands in a brain that is ready to receive it.
A patient who spends the hour before your session sitting alone in a hospital room watching television is not in the same neurochemical state as a patient who spent that hour in a brief social interaction, a short walk, or doing something that made them feel capable.
The sequence matters. What happens before your session is part of your intervention whether you designed it that way or not. A clinician who understands this designs the conditions before the session begins, not just the activities within it.
This is the piece that is missing from almost every rehabilitation plan across every discipline. The physical therapist designs the exercise. The speech pathologist designs the strategy. The occupational therapy practitioner designs the activity. Nobody designs the neurochemical context that determines whether any of it will be retained🔥.

How to Treat This (Real Sessions)
Before the session: Build a brief activation sequence into your session opening. This does not require extra time. It requires intentionality.
A two-minute conversation about something your patient cares about activates the reward system before a single therapeutic task begins. Ask about their grandchildren. Ask about the sport they used to play. Ask what they are looking forward to. The dopaminergic response to anticipated reward begins before the reward occurs. You are priming the learning system by engaging the anticipatory circuit.
A short movement burst before a cognitive task (even two minutes of standing, walking in the hallway, or marching in place) elevates dopamine and norepinephrine simultaneously. This is not warming up. This is neurochemical preparation. The evidence base for exercise-induced cognitive priming is substantial and directly applicable to your pre-session design regardless of your discipline.
During the session: Tie every task to a functional destination the patient named themselves. Not a destination you identified. Not a destination written in the chart. One the patient told you matters to them.
The basal ganglia are exquisitely sensitive to the relevance signal. Goal-directed behavior that the patient has personally endorsed activates the dopaminergic circuit more reliably than therapist-assigned tasks performed for compliance. This is why a patient who cannot retain a ten-step home program can remember exactly how to make their grandmother's recipe. The relevance signal is doing the neurological work.
Structure small wins deliberately. Each successful completion of a meaningful task generates a dopamine response that primes the next attempt. This is not positive reinforcement in the behavioral sense. It is sequential neurochemical preparation. Design your session so that the first task is achievable, the second is slightly harder, and each completion builds the chemical momentum for the next.
Do not end the session at the hardest point. The brain consolidates what it last experienced successfully. A session that ends in failure or frustration consolidates a failure trace. A session that ends with a meaningful accomplishment (even a small one!) closes on a dopamine signal that supports overnight consolidation and next-session readiness.
Across Disciplines
PT: Exercise is a dopamine intervention. You have been doing this all along without calling it that. A ten-minute walk before a balance or strengthening session is not a warmup. It is neurological preparation. The motor learning that follows is happening in a brain that is more chemically ready to encode it. Name it that way to your patient. It changes how they experience the effort.
SLP: Conversation about a meaningful topic before a speech or cognitive-communication task is not rapport building. It is dopaminergic priming. The language and memory systems you are targeting activate more robustly when the reward circuit is engaged first. Your session structure is a neurological sequence. Design it as one.
OT: Meaningful occupation is not your philosophical framework. It is your mechanism of action. When your patient engages in an activity connected to their identity and their roles, the dopaminergic response is the reason the intervention works. You have always known this. Now you have the neuroscience to say it plainly to every other discipline in the building.
Documentation
Identify and document:
- neurochemical readiness indicators: initiation quality, affect at session onset, carry-over from prior session, patient-reported engagement in meaningful activity outside of therapy
- session design rationale: why the session was structured in a specific sequence, what activation strategy was used prior to skill-based tasks, and how task selection was tied to patient-identified meaningful roles
- dopamine-relevant lifestyle factors: sleep quality, social engagement, physical activity between sessions, presence of meaningful daily activity , all of which directly affect learning readiness
- response to activation sequence: whether pre-session priming produced observable changes in initiation, engagement, or performance quality
Do not write: patient participated in therapeutic activity with moderate assist. Carry-over from prior session was limited.
Write what actually happened:
Patient presented with flat affect and slow initiation at session onset, consistent with low neurochemical readiness for learning. Pre-session activation sequence implemented: two-minute conversation regarding patient-identified meaningful role as primary caregiver, followed by three-minute hallway ambulation. Observable improvement in initiation speed and verbal engagement noted following activation sequence. Skilled therapeutic activity then introduced, tied directly to patient-identified goal of returning to meal preparation for family. Task completion with one verbal cue. Patient verbalized connection between session activity and functional goal. Session closed with successful task completion to support consolidation. Lifestyle factors affecting dopaminergic readiness discussed: sleep disruption reported, social isolation noted, referral to recreational therapy placed. Carry-over expected to improve as neurochemical conditions are addressed alongside skill-based practice.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!
What's included:
[Resource 1] Brain Training, Lifestyle, and Dopamine - Patient-Facing Handout for Guided Patient Education on how dopamine impacts daily life and lifestyle ideas to implement it.
[Resource 2] Basal Ganglia Patient Handout - Clinician-Facing and Patient-Facing resource for understanding the neural substrate behind everything discussed in this issue.
Handout 1: Brain training, Lifestyle, and Dopamine
This is your patient-facing education resource for this issue. Use it to explain why what your patient does between sessions matters as much as what happens during them. A patient who understands that sleep, social interaction, movement, and meaningful activity are not lifestyle suggestions but neurological prerequisites for learning will approach their rehabilitation differently.
Clinical tip: Use the low versus high dopamine comparison on page one to help your patient self-identify where they are right now. Ask them to point to which list describes their typical day. That self-assessment is your opening for a direct conversation about lifestyle as a clinical target.
Dopamine and Parkinson's Disease - Patient Resource
Dopamine and Parkinson's Disease - Clinician Resource
Handout 2: Basal Ganglia Patient Handout
This is your clinician-facing and patient-facing resource for understanding the neural substrate behind everything discussed in this issue. The basal ganglia are the system through which dopamine modulates learning, habit formation, initiation, and motivation. When this system is compromised through Parkinson's disease, stroke, TBI, or any condition affecting subcortical structures,the neurochemical conditions for learning are structurally disrupted, not just situationally low.
Clinical tip: Use this handout when your patient or their family is asking why therapy is not producing the carry-over they expected. The answer is often in this document. A damaged basal ganglia circuit is not simply a movement problem. It is a learning and motivation problem. That reframe changes the family's expectations, increases their support for lifestyle interventions, and reduces the pressure on both patient and clinician to produce results that the neurological substrate cannot yet support.
One-Line Clinical Reasoning Starters
Low Neurochemical Readiness at Session Onset
- Low neurochemical readiness identified at session onset based on flat affect, slow initiation, and absent carry-over from prior session
- pre-session activation sequence implemented to prime dopaminergic circuit prior to skill-based task introduction
- session structure modified to support learning consolidation rather than task volume.
Meaningful Role as Task Anchor
- Patient-identified meaningful role incorporated as primary task anchor
- goal-directed activity tied to personally relevant functional destination to activate basal ganglia reward circuitry and support dopamine-dependent encoding during skilled intervention
Lifestyle Factors Disrupting Learning Readiness
- Lifestyle factors disrupting neurochemical learning readiness identified: sleep disruption, social isolation, and absence of meaningful daily activity reported
- patient education provided regarding dopaminergic impact on carry-over and retention
- referrals placed and home program modified to incorporate dopamine-supportive activities between sessions.
Deliberate Session Closure Strategy
- Session closed with successful meaningful task completion to support overnight consolidation of skilled practice
- ending session on achievement rather than maximum challenge is a deliberate neurological strategy, not a scheduling accommodation.
Exercise-Based Pre-Session Priming
- Exercise-based pre-session priming implemented prior to cognitive and motor skill practice
- evidence-based strategy to elevate dopamine and norepinephrine prior to learning-dependent tasks
- response to priming documented as baseline for session structure progression.
See you in the next newsletter

Responses