
A couple of friendly reminders:
- This is not medical advice. The content of this Newsletter is informational only.
- working memory <-- Yellow highlighted text are helpful links for you to click on.
- Member only content is at the bottom of the newsletter where you will receive...
- relevent links to resources and/or printables from the BOT Google Drive. If you are a member and have not been added to the drive for content, please request access by clicking this link.
- Clinical conversation starters that take you a bit deeper than the documentation tips in this newsletter.
- If you want to learn more about the Functional Cognition Lab inside the BOT Portal, click here.
Picture This:
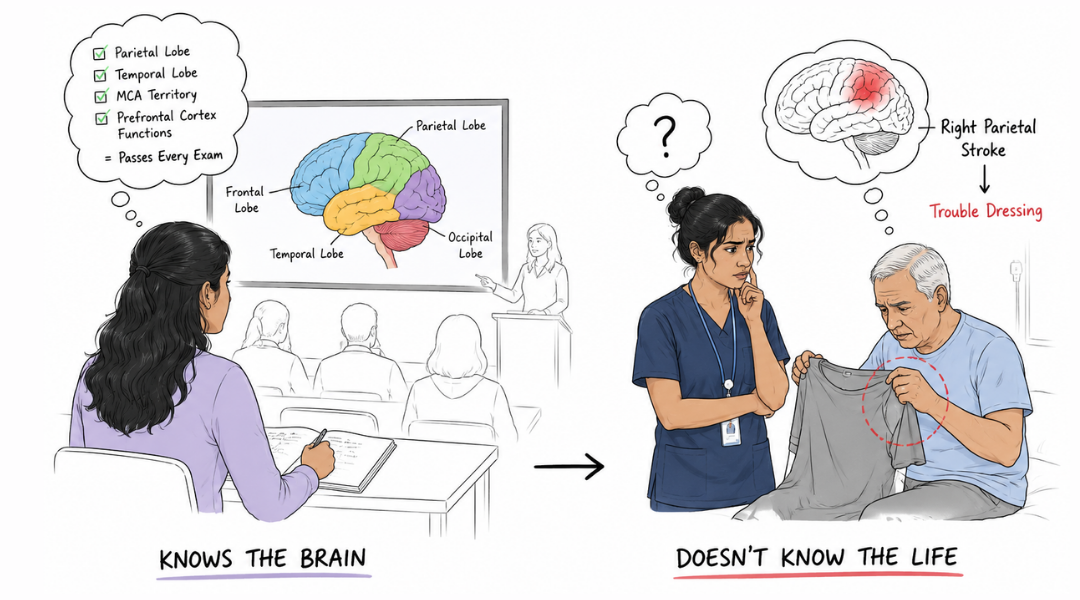
She sits in the back row of her neuroanatomy course with a perfectly color-coded brain diagram in front of her.
She can label the parietal lobe. She can label the temporal lobe. She can tell you which artery supplies the middle cerebral territory and recite the functions of the prefrontal cortex from memory. She passes every exam.
Six months later she is in her first clinical rotation and her supervisor asks her why the patient with the right parietal stroke is having trouble dressing himself.
She does not know.
Not because she did not study. Because nobody ever connected the label to the life. Nobody stood in front of that diagram and said: this is the region that tells your brain where your body is in space, where objects are in relation to you, and how to direct your hands toward a target with accuracy. When this region is disrupted, your patient will not be able to find the armhole. Not because they are confused. Because the spatial map that guides that movement no longer exists in the way it did before.
She learned the brain. Nobody taught her how to use it.
Now, Picture This:
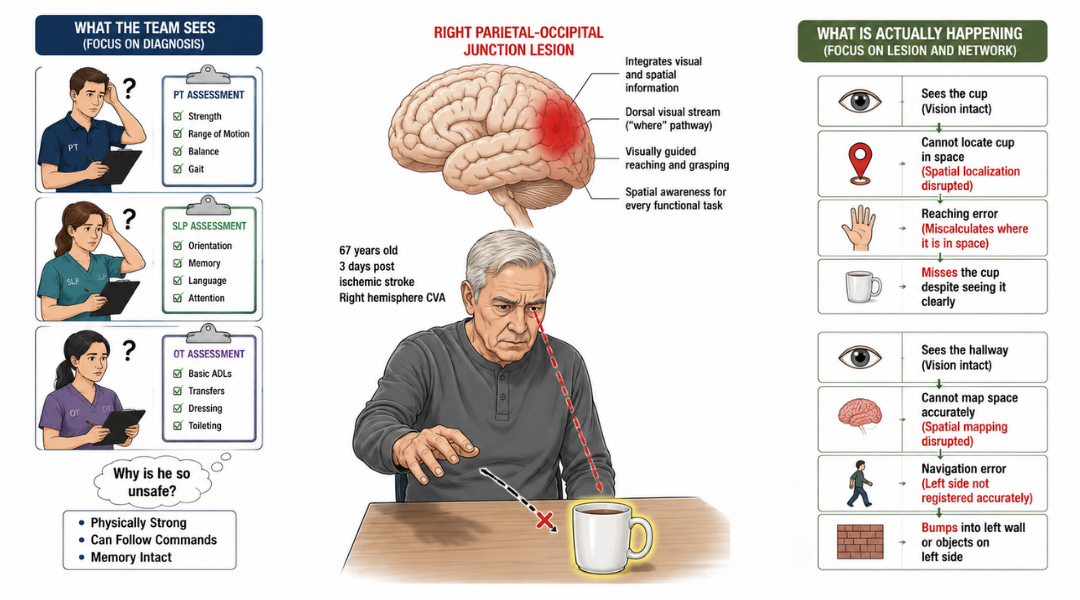
He is 67 years old. He had an ischemic stroke three days ago involving the right parietal-occipital junction. The imaging report says right hemisphere CVA. The team says stroke protocol. Everyone begins their evaluation.
The PT assesses strength, range of motion, and gait. The SLP screens orientation and memory. The OT evaluates ADL performance.
Nobody asks what lives at the parietal-occipital junction. Nobody considers that this specific region integrates visual and spatial information, governs the dorsal visual stream responsible for locating objects in space, supports the coordination of visually guided reaching and grasping, and contributes to the spatial awareness that makes every functional task possible.
He is treated like a stroke. Not like a man with a specific lesion in a specific region with a specific set of disrupted networks that require a specific clinical response.
Two weeks later the team is puzzled. He is physically strong. He can follow commands. His memory seems intact. But he cannot find his cup on the table even when it is directly in front of him. He reaches for objects and consistently misses. He cannot navigate the hallway without bumping into walls on his left side. He is being labeled as confused and unsafe.
He is not confused. His dorsal visual stream is disrupted. His brain can see the cup. It cannot locate it in space.
That is not a generic stroke finding. It is a structure-function finding. And if nobody on your team was ever taught to think that way, nobody will treat it that way.
What is actually happening:
Neuroanatomy courses teach structure. Functional courses teach intervention. Almost nothing bridges the two in a way that is clinically actionable (this is not the case in all courses, everywhere. This is just an example for the majority of people who can agree that this is a gap in learning). The consequence of that gap is a profession full of skilled clinicians who treat diagnoses instead of disrupted systems.
This matters more than ever because neuroscience now understands things differently about brain injury and that understanding has changed the clinical picture entirely.
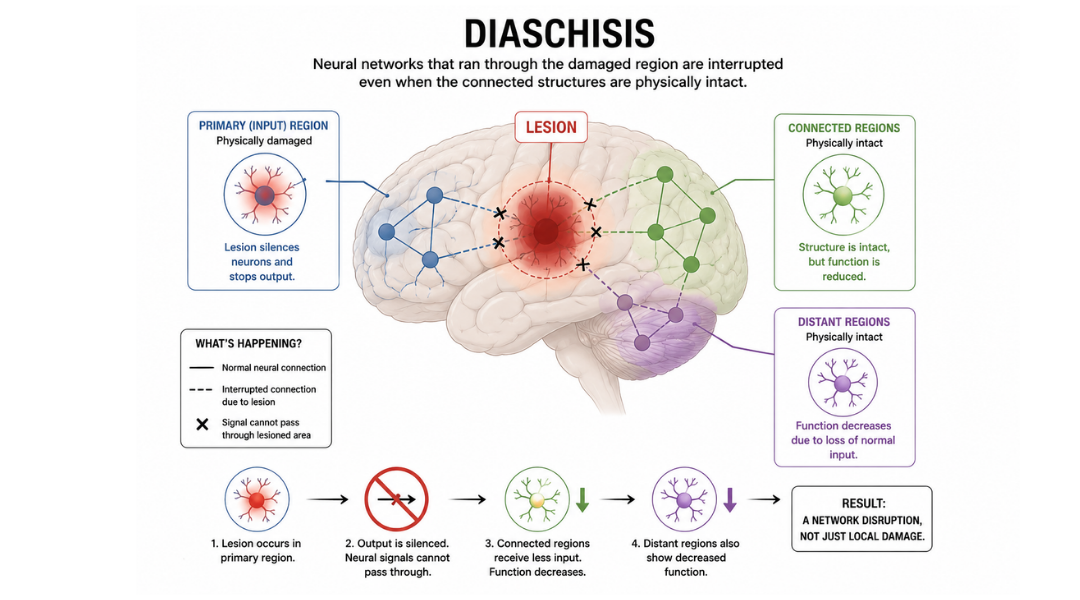
When a stroke occurs, the damage is not limited to the lesion itself. The perilesional zone ( aka the tissue surrounding the injury) is laden with inflammation, metabolic disruption, and structural disconnection.
Neural networks that ran through the damaged region are interrupted even when the connected structures are physically intact. This is called diaschisis which is when distant brain regions functionally degrade because their primary input source has been silenced.
What this means clinically is that your patient's deficits are not explained by the lesion alone. They are explained by the network disruption the lesion caused. And you cannot target a disrupted network if you do not know what the network does, where it lives, and what its functional signature looks like when it fails.
A parietal-occipital lesion does not just cause vision problems. It disrupts the dorsal visual stream, impairs visuospatial processing, degrades spatial attention, and compromises the visually guided motor planning that underlies nearly every functional task a human performs. That is not a generic stroke presentation. It is a specific network failure with a specific clinical footprint.
Name it. Then you can tame it.
The frontal lobe handout and the symptoms by lobe handout at the end of this issue exist for exactly this purpose 🧠. They are not study tools. They are clinical translation resources. The gap between what is on those diagrams and what your team is documenting in the chart is the gap this newsletter is asking you to close.
Take Action
Four clinical habits that bridge structure to function:
1. Read the imaging report for location, not just diagnosis.
Right hemisphere CVA tells you almost nothing clinically useful. Right parietal-occipital ischemic infarct tells you exactly where to look, what to measure, and what to expect. If your team does not have access to imaging, ask. If nobody has read it, read it. Location is your first clinical data point.
2. Map the lesion to the lobe before you choose your assessment.
Before you select a single standardized measure, ask what functions live in the affected region and which of those functions your assessment actually captures. A generic cognitive screen administered to a patient with parietal involvement will miss the spatial processing deficits entirely. Your assessment is only as precise as your anatomical reasoning.
3. Distinguish what the patient cannot do from why they cannot do it.
Cannot dress independently is an observation. Cannot locate clothing items in space due to disrupted dorsal visual stream processing is a clinical finding. The first leads to compensatory strategy training. The second leads to targeted intervention at the level of the disrupted system. They are not the same treatment.
4. Teach what you know to your team.
Structure-function reasoning does not belong only in the OT note or the SLP evaluation. It belongs in the team meeting, the family conference, and the discharge plan. If you are the clinician who understands why this patient's presentation looks the way it does, say it out loud where everyone can hear it.
The setup:
Before your next evaluation of a patient with any neurological diagnosis, do this.
Pull the diagnosis or imaging report. Identify the primary region of involvement. Open the lobe function reference at the end of this issue. List the functions attributed to that region. Then ask: which of those functions am I actually measuring? Which of those functions is my intervention targeting? Which of those functions has nobody addressed yet?
That gap between the list and your current plan is your clinical opportunity. It is also the argument for why structure-function reasoning is not an academic exercise. It is a precision clinical skill that changes outcomes.

How to Treat This (Real Sessions)
We are using parietal-occipital involvement as the clinical example throughout this newsletter because it crops up so often in my clinical practice :-)
What parietal-occipital disruption actually looks like in your session:
- The patient reaches for objects and consistently misses or overshoots.
- They lose track of objects that are directly in front of them.
- They have difficulty navigating space even when physically capable of the movement.
- They cannot reliably locate body parts in relation to their environment.
- They struggle with any task that requires coordinating vision with action (dressing, grooming, meal preparation, transfers, or almost every type of occupation).
- They are fatigued faster because their brain is compensating for these network-wide disruptions in order to keep up with clinician-guided demands.
None of this will show up on an orientation screen. Very little of it will show up on a standard cognitive assessment.
All of it is a direct functional consequence of disrupted visuospatial processing in the dorsal visual stream.
Across Disciplines
PT: Your patient is not unsafe because they are weak or because their balance is globally impaired. They are unsafe because their brain cannot accurately locate their body in space relative to the environment around them. Your gait training needs to explicitly address spatial navigation, not just lower extremity mechanics. Add visuospatial demands to your mobility tasks deliberately. Document the spatial processing deficit as the primary safety barrier, not generalized fall risk.
SLP: Your patient's word retrieval and memory deficits may be compounded by spatial attention disruption affecting their ability to orient to and process incoming information. Left neglect in a right hemisphere stroke is not an attention problem in the conventional sense. It is a spatial representation failure. Your cognitive-communication treatment needs to account for where in space your patient can reliably process information and build from there.
OT: Every ADL task your patient performs requires the dorsal visual stream to locate objects, orient the hand, and guide the movement to completion. When this stream is disrupted, adaptive equipment and verbal cueing are insufficient as primary interventions. Your treatment needs to directly address visuospatial processing at the task level, not compensate around it indefinitely. Start with the spatial demands of the task before you address the motor demands.
Across all disciplines: The perilesional inflammation that surrounds a subacute stroke lesion is not static. The network disruption it causes is most severe in the first weeks and can improve substantially with targeted input to the affected systems. This is your window. Precise, system-targeted intervention during the subacute phase capitalizes on neuroplasticity in a way that generic rehabilitation does not.
Know the region. Target the system. Document the network. Treat the window.
Documentation
Identify and document:
- lesion location and functional implications: specific region involved, primary functions attributed to that region, and how those functions map onto the patient's observed deficits
- network disruption: which functional systems are likely compromised beyond the lesion itself, including perilesional and diaschisis-related dysfunction
- assessment precision: which standardized measures were selected specifically to capture the affected functions, and which deficits may not be captured by standard screening tools
intervention rationale: how the treatment plan targets the disrupted system specifically rather than the functional limitation generically - treatment window: documentation that the subacute neuroplasticity window is being actively leveraged through system-targeted intervention
Do not write: patient presents with right CVA with deficits in ADL performance and safety awareness. Skilled OT indicated.
Write what actually happened:
Patient presents with right parietal-occipital ischemic infarct with disruption to the dorsal visual stream and visuospatial processing networks. Observed deficits consistent with lesion location include consistent overshooting during reach-to-grasp tasks, inability to locate objects in near space without tactile cueing, and spatial navigation failure during ambulation in a familiar environment.
Standard cognitive screening administered; results do not capture visuospatial processing deficits specific to lesion region. Supplemental visuospatial assessment selected to characterize spatial attention and visually guided motor planning deficits. Intervention plan targets dorsal stream processing directly through graded visuospatial tasks in functional contexts.
Perilesional neuroplasticity window identified as treatment rationale for intensive, system-targeted approach during subacute phase. Skilled OT indicated to address structure-specific network disruption with precision.
Education That Matters
The gap between neuroanatomy education and clinical application is not simply a curriculum problem. It is a reflection of where rehabilitation science has historically positioned itself which is downstream of the injury, focused on compensating for deficits rather than targeting the disrupted systems that produced them.
That positioning is changing.
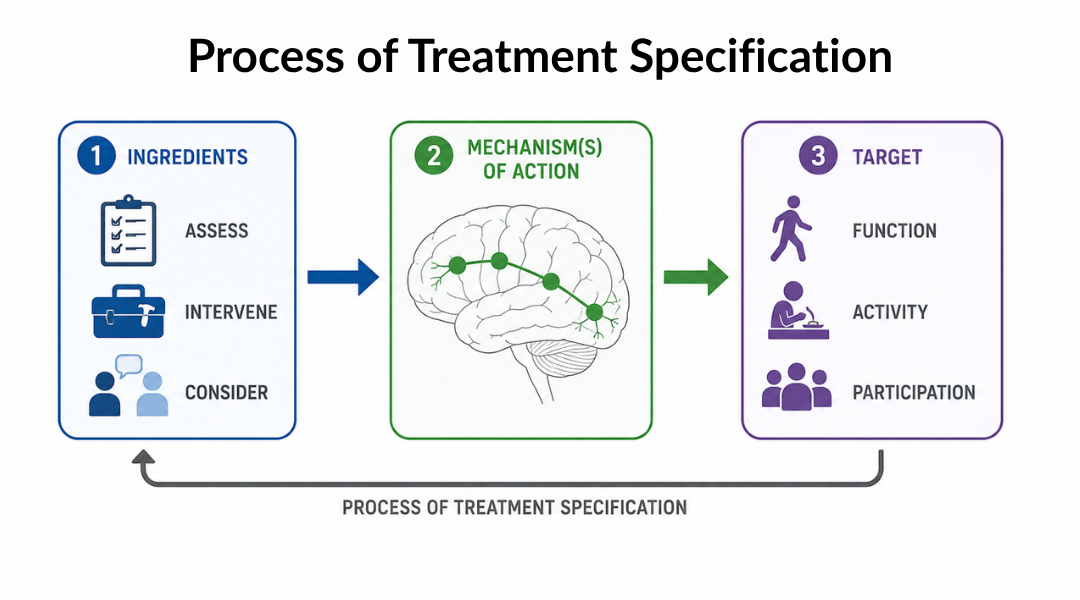
Rehabilitation Treatment Specification System, or RTSS, is a framework developed to bring precision and specificity to rehabilitation intervention design. Its core argument is that effective rehabilitation requires clinicians to identify the specific mechanism of the deficit, target that mechanism directly with a theoretically grounded intervention, and evaluate change at the level of the mechanism, not just the functional outcome. RTSS does not allow a clinician to say the patient has difficulty with ADLs and leave it there. It requires the clinician to name what is broken, why it is broken, and what the intervention is doing to fix it.
This is structure-function reasoning operationalized as a treatment framework. It is precisely what the student in the back row of the neuroanatomy course was never taught to do, and precisely what the team treating the parietal-occipital stroke patient failed to apply.
Precision rehabilitation extends this argument further. It proposes that rehabilitation outcomes can be optimized when interventions are matched to the specific biological, neurological, and behavioral profile of the individual patient, not applied uniformly based on diagnosis category. A stroke is not a treatment target. A disrupted visuospatial processing network in a 67-year-old man three weeks post-ischemic infarct in a specific vascular territory is a treatment target. The difference between those two framings is the difference between generic rehabilitation and precision rehabilitation.
For student clinicians and educators reading this: the neuroanatomy you are learning or teaching is not background knowledge. It is the clinical reasoning infrastructure that precision rehabilitation requires. The functions on the lobe diagram are not facts to memorize for an exam. They are the vocabulary of a clinical language that allows you to name what is disrupted, target it directly, and measure whether your intervention reached it.
If we do not teach it that way, nobody will apply it that way.
And that is a cost our patients cannot afford.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!
What's included:
[Resource 1] General Functions Within Major Regions of the Cerebral Cortex Handout
[Resource 2] Symptoms Associated with Each Lobe Handout
Handout 1: General Functions Within Major Regions of the Cerebral Cortex
This is your clinical translation reference for structure-function reasoning at the bedside. Use it before your evaluation to identify which functions are attributed to the region of involvement, and use it in team meetings to anchor your clinical reasoning in neuroanatomical specificity.
Clinical tip: Do not use this handout as a checklist. Use it as a question generator. For each function listed under the affected lobe, ask: am I measuring this? Am I treating this? If the answer to both is no, you have identified a gap in your plan.
Handout 2: Symptoms Associated with Each Lobe
This is your deficit-mapping reference. When your patient presents with a symptom you are struggling to explain, start here. Match the observed behavior to the lobe. Then go back to the lesion location and ask whether the geography of the injury accounts for what you are seeing.
Clinical tip: Use this handout in student supervision and case conferences. Present a patient's observed deficits without naming the diagnosis or lesion location and ask the team to identify which lobe the presentation points to. That exercise builds the structure-function reasoning muscle that neuroanatomy courses rarely develop explicitly.
Hemmorrgic Stroke vs Ischemic Stroke Handout
Common Symptoms of CVA by Artery
One-Line Clinical Reasoning Starters
Structure-Function Deficit Identification
- Lesion location mapped to functional systems prior to evaluation
- deficits observed consistent with disruption to identified region
- assessment selection modified to capture region-specific functions not addressed by standard cognitive screening
- skilled intervention indicated to target disrupted system directly.
Perilesional Network Disruption
- Perilesional inflammation and network diaschisis identified as contributing factors to functional deficits beyond the lesion boundary
- intervention plan designed to target affected networks during subacute neuroplasticity window
- system-specific treatment rationale documented to support skilled care intensity.
Visuospatial Processing Deficit — Parietal-Occipital Involvement
- Dorsal visual stream disruption identified secondary to right parietal-occipital ischemic infarct
- visuospatial processing deficit documented as primary mechanism underlying reach-to-grasp errors, spatial navigation failure, and object location impairment
- skilled intervention targeting visuospatial system directly rather than compensating generically for ADL dependence.
Assessment Precision Gap
- Standard cognitive screening administered
- results do not capture visuospatial or region-specific deficits attributable to lesion location
- supplemental assessment indicated to characterize disrupted functions specifically
- treatment plan cannot be adequately designed from generic screening data alone.
Student Clinician or New Graduate Supervision Note
- Structure-function reasoning explicitly incorporated into supervision framework
- student demonstrated ability to map lesion location to functional systems and generate assessment and intervention rationale grounded in neuroanatomical specificity
- clinical education targeted at bridging neuroanatomy coursework to precision rehabilitation application.
See you in the next newsletter

Responses