When the Scores Don't Match the Person: Using Activity Analysis to Bridge Cognitive Capacity and Functional Performance
Jul 07, 2026
When the Scores Don't Match the Person: Using Activity Analysis to Bridge Cognitive Capacity and Functional Performance
Michelle C. Eliason, MS, OTR/L and Adrianna M. Brown, MS, OTR/L
Key Words: activity analysis, cognitive load, functional cognition, mild cognitive impairment, occupational performance
Define Cognitive Remedial Therapy
In outpatient occupational therapy, cognitive remedial therapy is a skilled, neuroscience-informed rehabilitation approach that targets the cognitive systems underlying functional performance. It is not limited to compensation, adaptation, or teaching a person to “work around” impairment. While compensatory strategies remain important, cognitive remedial therapy also uses the principles of neuroplasticity, motor learning, attention, memory, executive function, and environmental demand to guide how intervention is designed, graded, and progressed.
This means treatment begins with the brain, but it does not stay abstract. The clinician identifies which cognitive processes are breaking down during meaningful activity, such as attention shifting, working memory, sequencing, spatial orientation, error monitoring, inhibition, or cognitive flexibility. Activity analysis is then used to translate those brain-based impairments into observable task demands. The occupation becomes the clinical arena where cognitive systems are challenged, supported, strengthened, and reorganized.
In this model, outpatient cognitive remedial therapy is more than worksheet practice, generic “brain games,” or environmental modification alone. It is the deliberate construction of therapeutic activities that place the right level of cognitive demand on the person at the right time. Tasks are graded to increase cognitive load, reduce unnecessary barriers, promote error awareness, strengthen strategy use, and support carryover into daily routines. The goal is not simply to make the task easier. The goal is to understand the cognitive architecture of the task and use that understanding to improve functional performance.
This article is written from that operational position. Cognitive scores matter, but they are not the whole story. Functional performance matters, but it must be analyzed with precision. Activity analysis allows occupational therapy practitioners to connect neuroscience to occupation by identifying where performance breaks down, why it breaks down, and how intervention can be built to directly address the cognitive systems involved. This is where outpatient cognitive rehabilitation moves beyond adaptation and compensation and becomes a skilled, brain-based, occupation-centered service.
A Familiar but Confusing Scenario
A 74-year-old man referred for outpatient occupational therapy following a mild traumatic brain injury scores in the moderate impairment range on standardized cognitive screening. His results suggest deficits in processing speed, working memory, and executive function significant enough to raise concern about his ability to manage daily tasks independently. Yet when you speak with him, he describes managing his morning medications without difficulty, preparing simple meals, and navigating his neighborhood independently. His wife confirms this. Nothing in his daily life looks like what the numbers predict.
This scenario is not unusual. Clinicians across rehabilitation settings encounter patients whose standardized cognitive scores appear inconsistent with their observed functional performance—sometimes patients perform better than expected, sometimes worse. The discrepancy is easy to dismiss or overcorrect. It is harder, and more clinically valuable, to understand.
The Gap Between Scores and Function
Standardized cognitive assessments are designed to isolate specific cognitive domains like attention, memory, executive function, and processing speed, and measure them under controlled conditions (Baum, Lau, Heinemann, & Connor, 2023; Lee, Lin, & Chiu, 2022). They are useful for identifying the presence and severity of impairment and for tracking change over time. What they cannot capture is how an individual performs within the complexity and variability of real-world occupational contexts (Gordon Muir Giles et al., 2025).
This creates a gap between cognitive capacity—what a person can do when assessed in a standardized environment—and functional performance—what a person actually does within the context of their daily occupations ("Occupational Therapy Practice Framework: Domain and Process-Fourth Edition," 2020). The Occupational Therapy Practice Framework: Domain and Process, Fourth Edition (OTPF-4) situates occupational performance at the intersection of the person, the environment, and the occupation itself. When clinicians focus exclusively on capacity-level scores, they risk incomplete, and sometimes inaccurate, clinical reasoning.
The consequences are real (G. M. Giles, Edwards, & Wolf, 2022; Toglia et al., 2017). Overestimating impairment can lead to unnecessary restrictions on independence. Underestimating it can leave patients without the supports they need. Intervention goals built solely on cognitive scores may target skills in isolation rather than addressing the performance breakdowns that actually limit participation in daily life (Gordon Muir Giles et al., 2025).
Why the Mismatch Happens
The mismatch between cognitive scores and functional performance reflects the dynamic nature of occupational performance. Individuals draw on multiple resources when engaging in activity, and deficits in one area may be offset, at least partially, by others.
Compensation is one of the most common contributors. A person with working memory impairment may rely on written lists, established routines, and environmental cues to complete tasks that would otherwise exceed their cognitive capacity. A person with slowed processing speed may have developed efficient, low-demand approaches to familiar tasks over decades. These compensatory strategies are often invisible in standardized assessment environments, which intentionally remove them.
Environmental supports play a similarly powerful role. A person who struggles in the novel, unstructured context of an assessment room may perform well in a familiar kitchen organized to meet their needs. Familiar environments reduce cognitive load by providing external structure—labeled cabinets, consistent object placement, predictable sequences—that reduces reliance on internal cognitive resources.
Task familiarity is the third major factor. Highly practiced activities, particularly those that have become procedural, require less deliberate cognitive processing than novel tasks. A person who has prepared the same breakfast every morning for forty years may complete that task with minimal working memory demand, even when working memory scores are significantly impaired.
These same factors explain performance breakdown. Compensation strategies fail under stress, fatigue, illness, or when the environment changes. A hospitalization, a home modification, or a caregiver change can eliminate the supports that sustained independence, and the cognitive impairment that was invisible in familiar routines suddenly becomes visible (Wiener & Pazzaglia, 2021).
Case Example
Consider a 68-year-old woman with a recent diagnosis of mild cognitive impairment (MCI) referred for an occupational therapy home evaluation. On the Montreal Cognitive Assessment (MoCA), she scored 19/30, with particular deficits in delayed recall and visuospatial function. The referring physician flagged concerns about safety with cooking and medication management.
During the home visit, she prepared a cup of tea and gathered her morning medications without hesitation. Her weekly pill organizer was filled and labeled in her own handwriting. Her kitchen was meticulously organized, with frequently used items at eye level and a handwritten schedule on the refrigerator.
What did not match: when asked to retrieve an item from a less familiar cabinet, she opened several wrong ones before finding it. When her phone rang mid-task during the evaluation, she lost her place in the medication sequence and could not confidently reconstruct it. Her competence was real, but contingent. It was supported by a specific, carefully maintained environmental structure and disrupted by any deviation from it.
Intervention focused not on remediating her memory but on mapping her existing compensation strategies, identifying the conditions under which they failed, and establishing additional supports—a second pill organizer for travel, a modified routine for managing interruptions—to extend her functional independence across a wider range of circumstances.
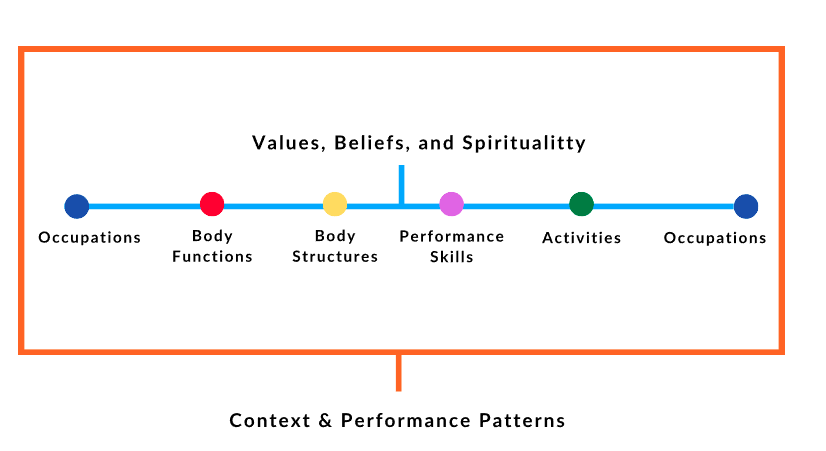
Figure 1. Activity analysis continuum illustrating occupation as both means and end. Client factors (values, beliefs, spirituality) and context and performance patterns anchor the whole-person framework within which body functions, body structures, and performance skills are addressed. Intervention begins and resolves at the level of occupation.
Activity Analysis as the Clinical Solution
Occupational therapy does not need a new framework to address the gap between cognitive capacity and functional performance. The profession already possesses the foundational method: activity analysis.
Activity analysis is the process of examining the component demands of an occupation including: what the task requires of the person physically, cognitively, emotionally, and socially, and how those demands interact with client factors and performance skills ("Occupational Therapy Practice Framework: Domain and Process-Fourth Edition," 2020). Rather than interpreting cognition in isolation, activity analysis situates cognitive processes within the specific, sequential context of meaningful tasks.
This shift in focus is more powerful than it may initially appear. When clinicians ask "What is this person's working memory score?" they obtain information about capacity. When they ask "Where in this task does the demand on working memory exceed what this person can reliably provide?", they obtain information about performance. The latter is directly actionable.
Applying It: Cognition Within Activity
Consider medication management, one of the most common functional cognition concerns in rehabilitation settings. A surface-level view treats this as a single task requiring "memory." Activity analysis reveals considerably more.
Opening a weekly pill organizer requires recognition of a familiar object (long-term procedural memory), identification of the correct day (orientation and working memory), and fine motor manipulation (motor planning). Filling the organizer from multiple prescription bottles requires sustained attention across multiple steps, inhibition of errors such as double-filling a slot, sequencing across bottles, and prospective memory to return to the task if interrupted. Taking the filled organizer's contents at the right time of day adds temporal memory and environmental cueing demands.
At each step, breakdown can occur for different cognitive reasons. A patient who consistently misses evening doses may have a prospective memory deficit, not a medication comprehension deficit. A patient who fills the wrong day's slots may have an orientation or visuospatial deficit. The appropriate intervention differs substantially depending on where in the task performance actually fails.
Intervention: Reducing and Grading Cognitive Load
Cognitive Load principles provide a clear and occupation-specific pathway for intervention. Occupational therapy targets cognitive load (i.e., the total demand a task places on a person's cognitive resources) through two complementary mechanisms: reduction and grading.
Cognitive load reduction involves modifying the task or environment to decrease demand to a level within the person's functional capacity. This includes simplifying multi-step processes, adding external cues such as visual schedules, labels, and alarms, restructuring the environment to reduce decision-making demands, and eliminating unnecessary steps. For our patient with MCI, repositioning frequently needed items to a consistent, visible location reduced the visuospatial and memory demands of her kitchen routine without changing the task itself.
Cognitive load grading involves systematically increasing task demands over time to build capacity, generalize skills, or expand the range of environments in which the person can function. This is distinct from repetition. Grading requires deliberate manipulation of task variables (e.g., adding a distracting stimulus, introducing an unfamiliar sequence, removing an environmental cue) and titrating difficulty based on observed performance, not on time elapsed or session count.
Together, these approaches allow practitioners to intervene directly at the point of performance breakdown while building toward meaningful occupational goals.
The Distinct Value of Occupational Therapy
Other disciplines assess cognition and provide important diagnostic and prognostic information. Occupational therapy provides something different: an understanding of how cognitive impairment manifests within the specific occupations that matter to a specific person in a specific context.
This is not simply a different setting for the same intervention. Occupation is not the backdrop for cognitive rehabilitation in occupational therapy, it is both the medium and the goal. Practitioners trained in activity analysis, environmental modification, and occupation-centered goal setting are positioned to identify performance breakdowns that standardized assessment cannot capture, design interventions that are ecologically valid, and measure outcomes in terms of meaningful daily life participation.
OTR and OTA Collaborative Roles
Within this process, role clarity between the occupational therapist (OTR) and the occupational therapy assistant (OTA) is essential ("Occupational Therapy Practice Framework: Domain and Process-Fourth Edition," 2020). The OTR is responsible for evaluating the relationship between cognitive capacity and functional performance, synthesizing standardized assessment data with clinical observation, and developing an occupation-centered intervention plan. The OTR establishes the clinical reasoning framework that connects cognitive findings to functional goals and determines the focus of activity analysis.
The OTA contributes through skilled implementation of the intervention plan, systematic observation of performance during activity, and documentation of responses to graded task demands across sessions. The OTA's direct observations during intervention often provide some of the richest available data about where and how performance breaks down in real time. The information gathered in colloaboration with an OTA informs ongoing OTR supervisory decision-making about plan modification and progression. This collaborative process produces a specific kind of skilled service that must be reflected accurately in documentation.
Documentation Example
CPT 97530 – Therapeutic Activity
Patient engaged in dynamic therapeutic activities targeting functional cognition deficits impacting safe participation in IADLs. Interventions focused on graded medication management simulation, sequencing of multi-step tasks, divided attention during interruption, error recognition, and problem-solving within real-life task demands. Patient demonstrated breakdown in task performance when external distraction was introduced, requiring verbal cueing for reorientation and step recall. Skilled OT services medically necessary to improve executive functioning, attention, and task completion required for independent home management. OTA reported observed performance data to supervising OTR to inform plan modification.
Moving Beyond Scores
Recognizing the distinction between cognitive capacity and functional performance is not a semantic exercise. It changes what practitioners look for, what they measure, and what they do. A clinician who understands this distinction will not dismiss a patient's reported independence because a score predicts otherwise, nor accept surface-level performance without examining its conditions and limits through quantifiable measures. When we adjust our perspective, a more accurate and clinically useful picture emerges. The picture identifies not just what a person cannot do, but where performance breaks down, why, and what can be done about it within the context of the occupations that define their daily life. Occupational therapy is uniquely positioned to start with scores and transform intervention to functional performance using activity analysis.
References
Baum, C. M., Lau, S. C. L., Heinemann, A. W., & Connor, L. T. (2023). Functional Cognition: Distinct From Fluid and Crystallized Cognition? Am J Occup Ther, 77(3). doi:10.5014/ajot.2023.050010
Giles, G. M., Edwards, D. F., & Wolf, T. J. (2022). Methodological Issues in Advancing the Status of Functional Cognitive Assessment. OTJR (Thorofare N J), 42(4), 253–259. doi:10.1177/15394492221116435
Giles, G. M., Goverover, Y., Foster, E. R., Connor, L. T., Farrar Edwards, D., Baum, C., & Toglia, J. (2025). Functional Cognition: Moving the Field Forward. OTJR: Occupational Therapy Journal of Research, 45(3), 399–407. doi:10.1177/15394492241296811
Lee, Y.-C., Lin, Y.-T., & Chiu, E.-C. (2022). A comparison of test-retest reliability of four cognitive screening tools in people with dementia. Disability and Rehabilitation, 44(15), 4090–4095. doi:10.1080/09638288.2021.1891466
Occupational Therapy Practice Framework: Domain and Process-Fourth Edition. (2020). Am J Occup Ther, 74(Supplement_2), 7412410010p7412410011–7412410010p7412410087. doi:10.5014/ajot.2020.74S2001
Toglia, J., Askin, G., Gerber, L. M., Taub, M. C., Mastrogiovanni, A. R., & O'Dell, M. W. (2017). Association Between 2 Measures of Cognitive Instrumental Activities of Daily Living and Their Relation to the Montreal Cognitive Assessment in Persons With Stroke. Arch Phys Med Rehabil, 98(11), 2280–2287. doi:10.1016/j.apmr.2017.04.007
Wiener, J. M., & Pazzaglia, F. (2021). Ageing- and dementia-friendly design: theory and evidence from cognitive psychology, neuropsychology and environmental psychology can contribute to design guidelines that minimise spatial disorientation. Cogn Process, 22(4), 715–730. doi:10.1007/s10339-021-01031-8