
A couple of friendly reminders:
- working memory <-- Yellow highlighted text are helpful links for you to click on.
- Member only content is at the bottom of the newsletter where you will receive...
- relevent links to resources and/or printables from the BOT Google Drive. If you are a member and have not been added to the drive for content, please request access by clicking this link.
- Clinical conversation starters that take you a bit deeper than the documentation tips in this newsletter.
- If you want to learn more about the Functional Cognition Lab inside the BOT Portal, click here.
Picture This:

Your patient has not done their home exercise program in three weeks.
You have gone over it four times. You printed the sheet. You demonstrated every exercise at the end of every session. You asked about it at the start of every session and watched them look at the floor.
You documented poor carry-over. You considered discharge. You wondered privately whether they actually want to get better.
They do. That is not the problem.
The problem is that you handed a ten-step independent action plan to a brain that cannot sequence, initiate, or sustain without external structure... and then measured compliance as though the neurological capacity for compliance was intact.
It was not.
This is not a motivation problem. It is an executive function problem. And you may be unintentionally ignoring it.
What is actually happening:
Executive function is the brain's management system. It lives primarily in the prefrontal cortex and governs everything that has to happen before and during a task including initiating, sequencing, monitoring, regulating, and adapting.
It is not a skill. It is the system that makes skills executable.
When it is impaired, your patient cannot reliably start tasks independently, sustain them without external cues, sequence multi-step procedures, regulate the emotional experience of difficulty, or monitor whether what they are doing is working.
A home exercise program requires all of those things simultaneously, every day, without you in the room.
This is not an OT-specific concern. If you have already read the Five Executive Functions in Practice series, you know what each component looks like in isolation. This issue is about what happens when those components are compromised and your patient is sitting in front of you... regardless of your discipline.
The speech pathologist whose patient cannot carry over their compensatory swallowing strategy at home is looking at the same problem as the physical therapist whose patient stops using their walker the moment they leave the clinic.
The executive system does not care what discipline issued the instruction. If it is impaired, the instruction will not stick.
How does this relate to the action you must take?
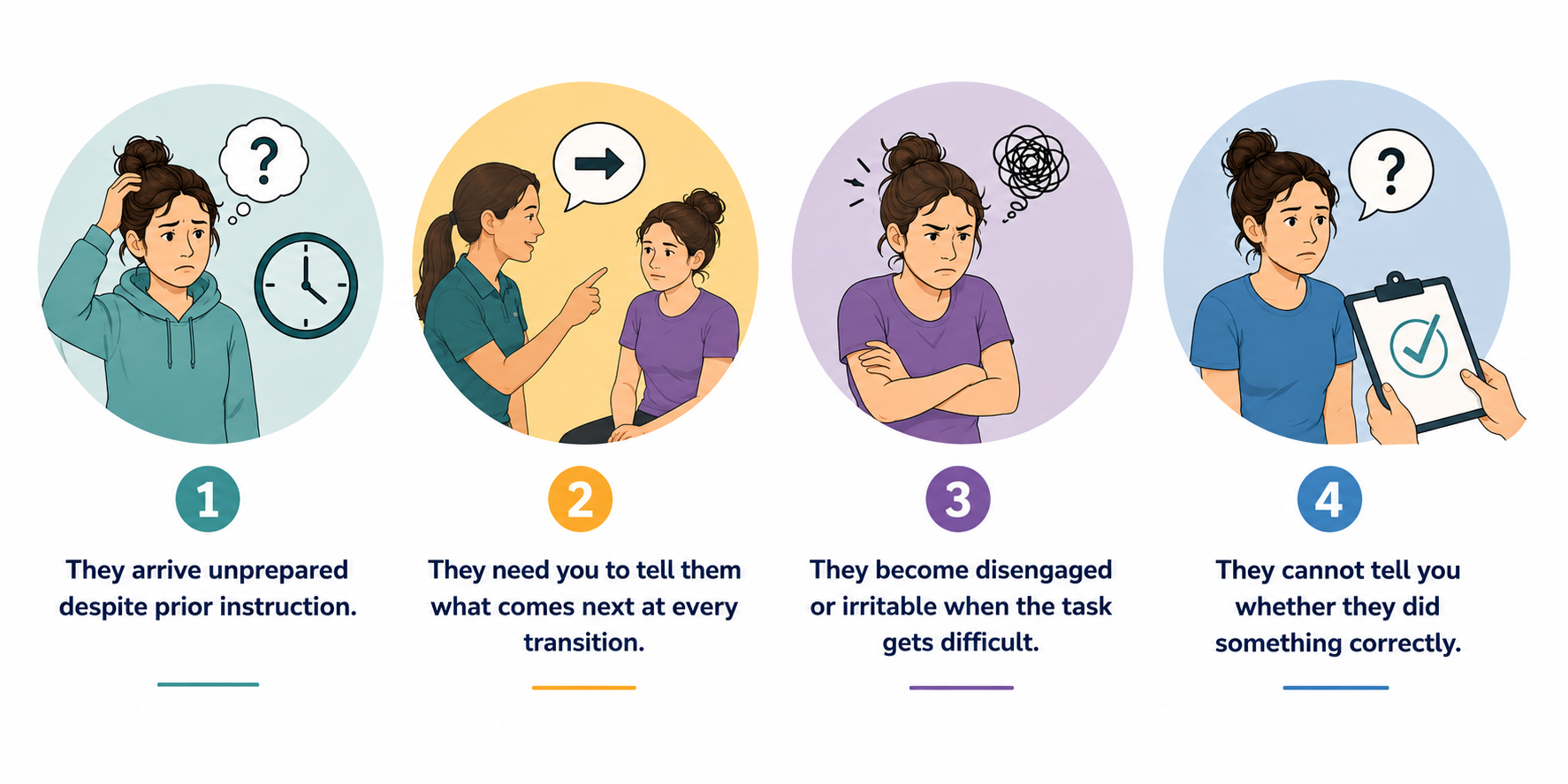
Before you redesign your intervention, you need to know whether Executive Function (EF) is the barrier. These are the four observable signs that the executive system is compromised before your session even begins.
1. They arrive unprepared despite prior instruction. No home program sheet. Forgot the appointment time. Cannot tell you what you worked on last session. This is not carelessness. It may be organization and working memory failure.
2. They need you to tell them what comes next at every transition. Between exercises. Between tasks. The moment you stop directing, they stop moving. The internal go-signal is not firing independently.
3. They become disengaged or irritable when the task gets difficult. Not laziness. Emotional regulation failure under cognitive load. The prefrontal cortex is managing too much and emotional regulation is the first system to drop.
4. They cannot tell you whether they did something correctly. They finish and look at you for confirmation rather than self-evaluating. Self-monitoring is offline. They are not being passive. They do not have access to the feedback loop.
Any one of these is a signal. All four is a clinical finding that belongs in your note and your treatment plan regardless of your discipline.
The setup:
You do not need a formal assessment to begin using this. You need to know what you are looking at before the session starts.
When your patient walks in, note three things before you say anything clinical:
- Did they bring what you asked them to bring?
- Do they reference anything from last session unprompted?
- How do they respond when you signal a transition?
That observation takes thirty seconds. It tells you whether the executive system is available for the session you planned or whether the session you planned needs to change before it begins.
If executive dysfunction is present, your intervention delivery changes. Not your goals. Your delivery.

How to Treat This (Real Sessions)
Identifying EF compromise changes how you structure every part of the session. Here is what that looks:
Initiation failure means the session needs external structure built in before the patient arrives.
- A visual schedule posted in the room.
- A checklist they reference independently.
- A consistent starting ritual that removes the demand to generate the first action from nothing.
Do not verbally prompt initiation and call it treatment. Build the structure that makes initiation possible and systematically remove it over time.
Sequencing failure means the home program cannot be a list. It has to be an environment.
- The exercise happens at the bedside because the bed is the cue.
- The swallowing strategy happens because the cup has a sticker on it.
- The walker gets used because it is the only thing between the patient and the bathroom door.
You are not simplifying. You are externalizing the sequence until the internal system can carry it.
Emotional regulation failure means your session environment is part of your intervention.
- How you greet the patient.
- How you respond when they struggle.
- Whether you signal frustration when they cannot recall something.
A dysregulated nervous system cannot learn. If your patient is dysregulated before the task begins, the task is not your first intervention. Co-regulation is.
Self-monitoring failure means verbal feedback at the end of the task is too late.
- Feedback has to be embedded. That is, a physical cue, a visual marker, a built-in pause where the patient evaluates before you respond. You are not withholding feedback. You are training the system that generates it internally.
Across Disciplines
PT: Your patient is not non-compliant with their fall prevention program. They cannot initiate a multi-step safety routine independently without an external trigger. The program needs an environmental anchor at the point of need, not more repetition in the clinic.
SLP: Your patient is not forgetting their swallowing strategy. They cannot self-monitor in real time under the cognitive load of a meal. The strategy needs to be embedded in the meal environment, not recalled from a verbal instruction given thirty minutes earlier.
OT: Your patient is not unmotivated. The internal management system that would drive their morning routine independently is not functioning. The routine needs to be built into the environment before it can be built into the person.
Documentation
Identify and document:
- executive function status: which components are compromised based on observed session behavior, not self-report alone
- initiation: latency to begin tasks, whether external cuing was required, how many transitions required prompting
- self-monitoring: whether the patient self-evaluated or sought external confirmation, error detection and correction rate
- emotional regulation: whether dysregulation was observed, at what point in the session, and what preceded it
- carry-over barrier: specific EF component identified as the primary barrier to home program follow-through
Do not write: patient demonstrated poor carry-over and limited motivation with home program.
Write what actually happened:
- Patient unable to recall home program components at session onset without clinician re-instruction, consistent with working memory impairment affecting independent task execution.
- Initiation failure documented at all within-session task transitions; external verbal cue required to resume activity.
- Emotional dysregulation observed when task difficulty increased, characterized by disengagement and task avoidance.
- Self-monitoring absent at task completion; patient sought external validation rather than self-evaluating.
- Executive function impairment identified as primary barrier to home program carry-over.
- Treatment plan modified to include external environmental structure, embedded feedback, and graduated reduction of clinician cueing.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!
What's included:
[Resource 1] What Is Executive Function - Patient-Facing Handout for Guided Patient Education
[Resource 2] Executive Skills Questionnaire Revised (ESQ-R)
Plus One Line Clinical Reasoning Starters
Handout 1: What Is Executive Function
This is your patient-facing education resource. Use it at the start of treatment before you assign a single home program item. A patient who understands that their brain has a management system (and that the management system is what is struggling, not their effort or their intelligence) enters the therapeutic relationship differently.
Clinical tip: Walk through the handout with the patient, do not hand it to them to read independently. Point to the component that matches what you observed in the four-sign screen. Name it plainly. Tell them what it means for how you are going to work together. That conversation is your first intervention.
What is Executive Function PDF
Handout 2: Link to Executive Skills Questionnaire Revised (ESQ-R)
The ESQ-R is a 25-item self-report measure assessing five areas of executive functioning: plan management, time management, organization, emotional regulation, and behavioral regulation. It is not a diagnostic tool. It is a structured conversation that tells you where to build external support first.
A patient who scores low on behavioral regulation needs a different session environment than one who scores low on plan management. A patient with emotional regulation deficits may disengage based entirely on how you respond when they struggle. The ESQ-R surfaces that information before your intervention design locks it out.
One important caveat: the ESQ-R depends on intact self-monitoring. If your patient cannot reliably self-monitor, you can use clinical observation or care-person interview.
One-Line Clinical Reasoning Starters
Executive function Impairment
- Executive function impairment identified as primary barrier to home program carry-over
- independent task execution requires intact initiation, sequencing, and self-monitoring, all of which are compromised
- skilled modification of intervention delivery required to build external structure commensurate with current executive capacity.
Initation
- Initiation failure documented at all within-session task transitions
- external verbal cue required at every transition
- Internal go-signal not activating independently
- skilled cueing hierarchy and graduated independence protocol indicated.
Emotional Regulation
Emotional dysregulation under cognitive load documented
Patient disengaged when task difficulty increased
Dysregulation identified as barrier to therapeutic participation
Session environment and task grading modified to reduce dysregulation threshold before skill-based intervention resumed.
Self-Monitoring
- Self-monitoring deficit documented
- Patient unable to evaluate own performance without external confirmation embedded real-time feedback system required within task design
- End-of-task verbal feedback insufficient as primary monitoring mechanism.
ESQ-R
- ESQ-R administered; results used to collaboratively identify executive strengths and deficit areas with patient
- Treatment plan structured to provide external support in identified deficit domains with systematic reduction of supports as independence increases.
See you in the next newsletter

Responses