
A couple of friendly reminders:
- working memory <-- Yellow highlighted text are helpful links for you to click on.
- Member only content is at the bottom of the newsletter where you will receive...
- relevent links to resources and/or printables from the BOT Google Drive. If you are a member and have not been added to the drive for content, please request access by clicking this link.
- Clinical conversation starters that take you a bit deeper than the documentation tips in this newsletter.
- If you want to learn more about the Functional Cognition Lab inside the BOT Portal, click here.
Picture This:
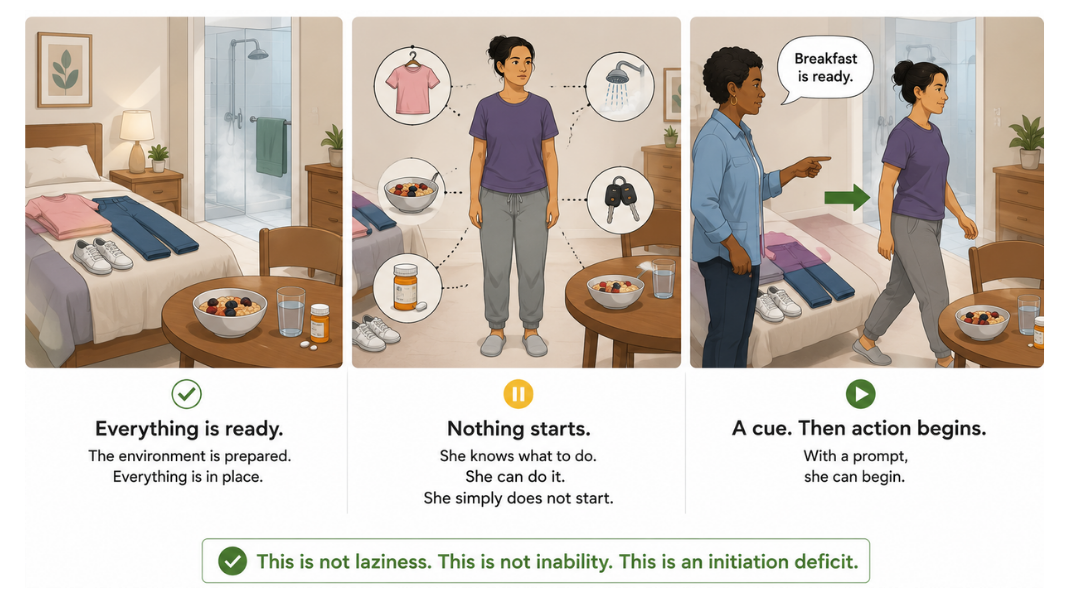
She sits down in the session chair and waits.
Not anxiously. Not impatiently. Calmly. As if she knows that in a moment, someone will tell her what to do...because someone always does.
At home, her caregiver lays out her clothes in the morning. Turns on the shower and tells her it is ready. Sets breakfast on the table and sits beside her. Reminds her to take her medication. Walks her through every step of every morning, not because she cannot do any of it, but because without the prompt, nothing begins.
Her physical capacity is intact. Her memory for how to do things is intact.
She can button a shirt, sort objects, walk across a room. She knows what needs to happen. She simply does not start.
Her family calls it laziness. Her chart calls it low motivation. Her last clinician wrote that she was 'unmotivated and dependent'.
👉 None of those are the right clinical frame.
This is an initiation deficit.
What is an initiation deficit?
The internal go-signal that should fire when a task needs to begin is not firing. And every external cue her caregiver gives her, every prompt her clinician provides, every verbal direction she receives is training that system to wait for the next one instead of generating its own.
The intervention for initiation is not more instruction. It is less. It is the deliberate removal of the external cue, the strategic silence that forces the internal system to activate or reveal exactly where it cannot.
This is the fifth and final newsletter in the Executive Functions in Rehabilitation series. It is also the one where the clinician does the least and the intervention is the hardest to execute, because doing nothing (i.e., staying quiet, not rescuing, not filling the silence) is a clinical skill that requires as much deliberate practice as any other.
What the activity actually is
The tools:
📋 A wall checklist — mounted at eye level before the patient enters the room. It reads: "Today you will complete:" followed by the number of stations listed, either in words or pictures depending on the patient's literacy and population. No other instructions appear on the checklist.
🔵 Station 1: Buttoning — four shirts laid flat on a table. Three have mismatched buttons — a button fastened into the wrong buttonhole, creating a misalignment the patient must detect, undo, and correct before completing the shirt. One shirt is correctly buttoned as a reference.
🟤 Station 2: Bead sorting — a pile of mixed-color beads on a table beside sheets of colored construction paper, one sheet per bead color. No instructions are posted. The patient must infer the task from the materials.
🍴 Station 3: Cutlery sorting — a mixed pile of plastic cutlery beside three empty containers. No instructions posted. The patient must infer that they are sorting by type.
🫘 Station 4: Bean bag transfer — bean bags on one side of the room, color-matched cones or polyspots on the other side. A sign posted at the station reads "Feet Only" with a picture of feet. The patient must move each bean bag to its matching cone using only their feet, mirroring the functional lower extremity movement needed to move objects out of the way in everyday environments.
📄 Station 5: Paper table — three sheets of paper on the table. One is a reading passage with a written response question. One is a word find. No verbal instructions are given. The patient must identify that both are meant to be completed and begin without direction.
⏱️ A timer — running from the moment the clinician stops speaking
📊 A tracking sheet: time to first initiation, number of spontaneous checklist returns, number of prompts required at each station, prompt type (verbal, gestural, proximity), validation-seeking behavior noted by station
The setup:
Stations are arranged around the room before the patient arrives. The wall checklist is mounted and visible from the door. When the patient enters and sits down, the clinician says one thing:
"There is a list on the wall that tells you what you will be doing today. I will be here if you need me."
Then the clinician stops talking. That is the instruction. Everything after that is the intervention.
👉 The clinician does not prompt. Does not gesture toward the wall. Does not fill silences. Does not answer questions about what to do next. If the patient asks what they should do, the clinician says: "Check the list." One time only. That is the entire verbal protocol.
Before the activity — lead with science, briefly
There is one thing to say to the patient before the session begins. Say it after you explain the list and before you stop talking:
"What we are working on today is your ability to start things on your own and trust that you know how to figure them out. Your brain knows how to do these things. We are training the part of your brain that gives itself permission to begin."
👉 That is not reassurance. That is encoding. A patient who understands they are training the starting system (not being tested on whether they can do the tasks) enters the silence differently than one who thinks they are failing a task they have not been told how to do.
Why the checklist is not the intervention
The wall checklist removes the planning demand. The patient does not have to generate what to do next...the list tells them. It does not remove the initiation demand. The patient still has to:
Look at the list. Decide to begin. Walk to the first station. Start the task without being told how. Finish. Return to the list. Choose the next station. Begin again.
👉 Every one of those moments is a discrete initiation event. There are at least ten in a five-station session. Each one requires the internal go-signal to fire independently.
- A patient who stands up and walks to station one without prompting has generated their first independent initiation.
- A patient who sits for four minutes before standing has given you a latency measure.
- A patient who stands, takes two steps, and then turns to look at the clinician has shown you that there is a disconnect at the moment of commitment, when the action shifts from intention to execution.
Document every one of these moments.
Why clinician silence is the active intervention
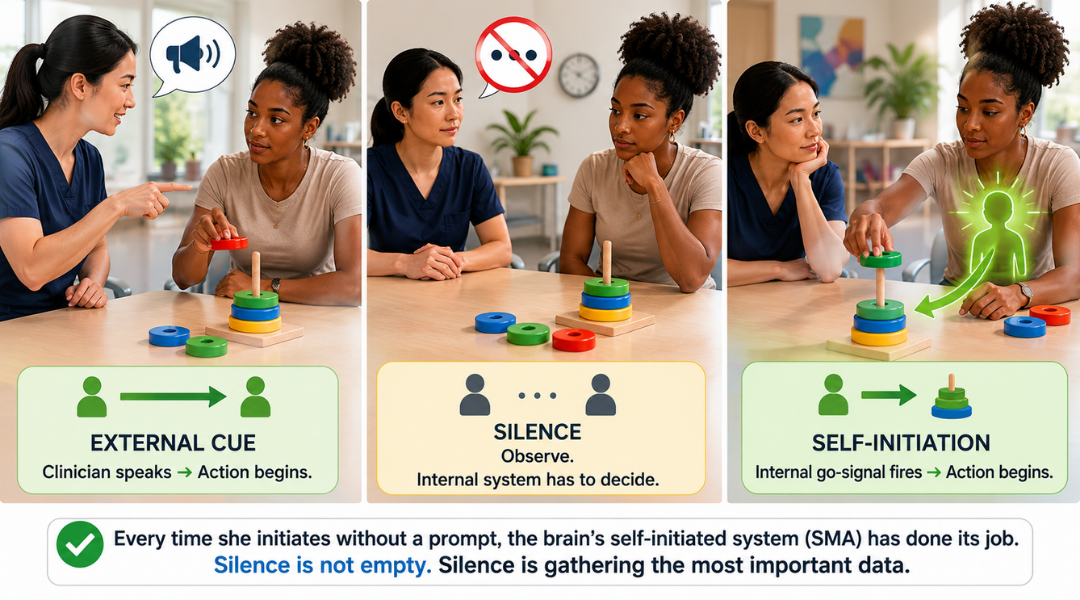
When the clinician speaks, the patient's nervous system relaxes. The external cue has arrived. The internal system does not need to fire because the signal came from outside.
When the clinician is silent, the internal system has two options: generate the go-signal independently, or wait. The patient who waits is not being passive. They are doing what their nervous system has learned to do; what years of external cueing have trained it to do. The wait is the learned response to the absence of direction.
👉 The supplementary motor area of the brain is specifically responsible for self-initiated movement, as distinct from externally-cued movement. It is more active before voluntary actions and less active when actions are triggered by an external signal. This distinction is not incidental, it is the neurological basis of why prompting a patient to begin is clinically different from waiting for them to begin themselves.
Every time the clinician stays silent and the patient initiates anyway, the supplementary motor area has done its job without external support. Every time the clinician speaks first, that system has been bypassed. Document which happened. It is the most important finding in the session.
Why the inference stations are a separate clinical demand
At stations 2, 3, and 4, the patient must figure out what they are supposed to do from the materials alone. No instructions are posted beyond the feet-only sign at station 4.
This adds a problem-solving layer on top of the initiation demand. A patient who walks confidently to station 2, stands at the bead table, and freezes has initiated but cannot infer. A patient who infers immediately but never approaches the table cannot initiate. Document which failure you observe. They point to different deficits and different intervention targets.
👉 The inference demand also tests confidence in self-directed action. The patient who looks at the bead table, makes an educated guess, and begins sorting without validation-seeking is demonstrating internal locus of control. The patient who approaches the table, looks back at the clinician, and waits for confirmation before touching anything is showing you exactly where the external validation dependency lives.
That moment "the glance back" is your most sensitive initiation and self-efficacy data point in the entire session. Note which station it occurs at, how many times per station, and whether it decreases across sessions.
Why this activity only works after rapport is established
This protocol requires the patient to tolerate uncertainty without becoming dysregulated. The silence, the ambiguous stations, the absence of direction...all of these are tolerable only when the patient trusts the environment they are in.
This is not a first-session activity. It is a session that happens after the patient has done several activities with you, knows the room, and has experienced success in your presence. The clinical relationship is the container that makes the silence safe rather than threatening.
👉 If you run this activity too early, you are not measuring initiation. You are measuring anxiety in an unfamiliar environment. Those are different clinical findings and they require different interventions. Build the foundation first. This session is the test of what has been built.

How to Treat This (Real Sessions)
⏱️ Start the timer the moment you finish your one instruction.
Do not start it when you think the patient should be starting. Start it when you stop speaking. The latency ["the pause"] between your last word and the patient's first movement toward the wall checklist is your primary initiation measure. Track it every session. Watch it decrease.
👉 Do not interpret long latency as non-compliance or confusion. Long latency is the clinical finding. It tells you exactly how long the internal system requires to generate a go-signal without external support. That number is what you are moving across this plan of care.
📋 When the patient returns to the wall checklist between stations
Note it, but do not acknowledge it. A nod, a smile, eye contact with meaning, all of these are external validation. The patient who seeks your face after checking the list and then looks away and moves to the next station anyway has generated their own internal permission. That is the clinical win. Do not celebrate it in the moment. Document it.
🔍 At the inference stations, wait through the full pause before offering any support.
If the patient stands at the bead table for two minutes without touching anything, that is two minutes of data. If they begin sorting incorrectly (e.g., beads in a pile not on the paper, cutlery mixed rather than sorted) let them continue. Error detection and self-correction at an inference station is a separate finding from initiation, and both belong in the note. Only intervene if the patient is about to leave a station without attempting it at all.
🗣️ The one permitted response to "What am I supposed to do?" is "Check the list." Said once. Calmly. Without elaboration.
If the patient asks a second time, the clinician remains silent. Document how many times the question was asked and at which stations. Repeated questioning is validation-seeking. It is your locus of control data.
📊 Track six variables every session:

(1) time to first initiation, (2) number of spontaneous checklist returns without prompt, (3) number of validation-seeking glances or questions by station, (4) number of stations completed without any clinician input, (5) prompt type if used, and (6) error self-correction rate at inference stations. They move independently and they tell different stories.
🔄 Grade by reducing the only permitted response.
- Early sessions: clinician may say "Check the list" once per station.
- Mid-protocol: clinician may say it once per session total.
- Late protocol: clinician remains silent for the entire session.
The progression from one permitted response to complete silence is your primary grading variable.
Document which level was active every session.
Documentation
Document the system,not just the task.
This is not a circuit training session.
Identify and document:
- initiation latency: time from last clinician word to first patient movement, every session
- self-directed action: number of stations initiated and completed without any clinician input, checklist return frequency, validation-seeking behavior by station
- internal locus of control: whether the patient proceeded after checking the list or waited for external confirmation, glance-back frequency, question-asking rate
👉 If you do not name it, it does not exist clinically.
Do not write "patient required verbal cues to initiate tasks."
Write what actually happened:
- initiation latency: 4 minutes 12 seconds from clinician's final instruction to patient's first movement toward wall checklist; no verbal prompt provided; patient initiated independently
- validation-seeking: patient returned gaze to clinician 3 times at station 2 (bead sorting) before beginning; clinician maintained neutral expression; patient proceeded without receiving confirmation; sorting completed correctly
- station 4 (bean bag transfer): patient read the sign, stood for 90 seconds, then began task using feet without prompting; self-correction observed when one bean bag was placed at incorrect cone; patient identified and corrected error without clinician input
- paper station: patient completed reading response but did not initiate word find; left table after first sheet; checklist not re-consulted before sitting down; clinician silence maintained
👉 Each of these is a specific, measurable, functionally meaningful clinical finding.
🧾 Tie it to function. Every note. Every session.
- morning routine initiation: beginning ADL tasks independently without caregiver prompt or verbal direction
- community participation: self-directing activity in environments where no one is telling them what to do next
- safety: initiating appropriate responses to unexpected situations without waiting for external direction
- caregiver burden reduction: decreasing the number of prompts required for the patient to complete their daily routine independently
👉 This is not a circuit activity.
👉 This is initiation and self-directed action training
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!
What's included:
[Resource 1] Station Setup Guide — your room setup reference with materials list, station configuration, the wall checklist template in both word-based and picture-based formats, and the feet-only sign for station 4. Print and laminate.
[Resource 2] Paper Station Sheets — your ready-to-print materials: one reading passage with a written response question targeting functional literacy and working memory, and one word find targeting visual perception, sustained attention, and working memory under self-directed conditions.
Handout 1: Station Setup Guide
Pull this before the patient arrives. Set up all five stations, mount the checklist, and have the tracking sheet ready before they enter the room. The session begins the moment you finish your one instruction. You will not have time to set up after that.
Clinical tip: The checklist format can be adapted to pictures depending the client. A patient who can read independently gets the word version. A patient with lower functional literacy or significant cognitive impairment gets the picture version.
Both versions communicate the same thing: here are the stations you will complete. Document which format was used and whether the patient referenced the checklist spontaneously or required redirection to it.
Handout 2: Paper Station Sheets
The reading and response sheet targets functional literacy and working memory: the patient reads a short passage and answers a written questions from memory without re-reading. The word find targets visual perception, sustained attention, and performance under self-directed time conditions.
Clinical tip: Do not pre-instruct the paper station. The patient must infer that both sheets are meant to be completed. Whether they complete one, both, or neither and in what order is your initiation and task persistence data. A patient who completes the word find but not the reading response has made a self-directed task selection. Document which sheet was initiated first, whether both were completed, and whether the patient left the station before finishing either.
Attention to Detail Activities
Full Cognition and Dual Tasking Google Drive
Visual Perception Google Drive
One-Line Clinical Reasoning Starters
Initiation latency of [X] minutes documented before first independent movement toward wall checklist
- external go-signal absent; internal initiation system required to activate without prompt
- skilled initiation training required to reduce latency toward functional independence threshold.
Validation-seeking behavior documented at [N] of 5 stations
- patient initiated tasks following glance-back to clinician without receiving verbal confirmation
- internal locus of control emerging; skilled facilitation of self-directed action required to reduce external validation dependency.
[N] of 5 stations completed without any clinician input
- [N] stations required [verbal / gestural / proximity] prompt
- skilled grading of permitted clinician response required to systematically reduce external cueing toward full self-directed session completion.
Inference failure documented at station [N]
- patient initiated approach but could not generate task from materials alone
- distinct from initiation deficit; skilled problem-solving facilitation required in addition to initiation training.
Initiation latency decreased from [X] to [X] minutes across [N] sessions
- measurable gain in internal go-signal activation documented
- direct functional correlate for independent morning routine initiation and reduction of caregiver prompting burden.
See you in the next newsletter

Responses