
Series Title: Structure-Function
A couple of friendly reminders:
- This is not medical advice. The content of this Newsletter is informational only.
- working memory <-- Yellow highlighted text are helpful links for you to click on.
- Member only content is at the bottom of the newsletter where you will receive...
- relevent links to resources and/or printables from the BOT Google Drive. If you are a member and have not been added to the drive for content, please request access by clicking this link.
- To go directly to the brand new structure-function folder in the BOT Google Drive for this series, click this structure-function link.
- Clinical conversation starters that take you a bit deeper than the documentation tips in this newsletter.
- If you want to learn more about the Functional Cognition Lab inside the BOT Portal, click here.
Picture This:

Your patient reaches for a cup of coffee on the counter. She does not overshoot. She does not spill it. Her hand slows and closes at exactly the right moment, before her eyes have even finished confirming the cup is there.
Three weeks post cerebellar stroke, that same reach looks different. Her hand travels too far, corrects, overshoots again in the other direction, corrects again. She is not weak. She is not confused about what a cup is. She is fully able to see the cup and name its location.
She just cannot predict where her hand will be half a second from now.
This is a cognition-related factor!
What is actually happening:
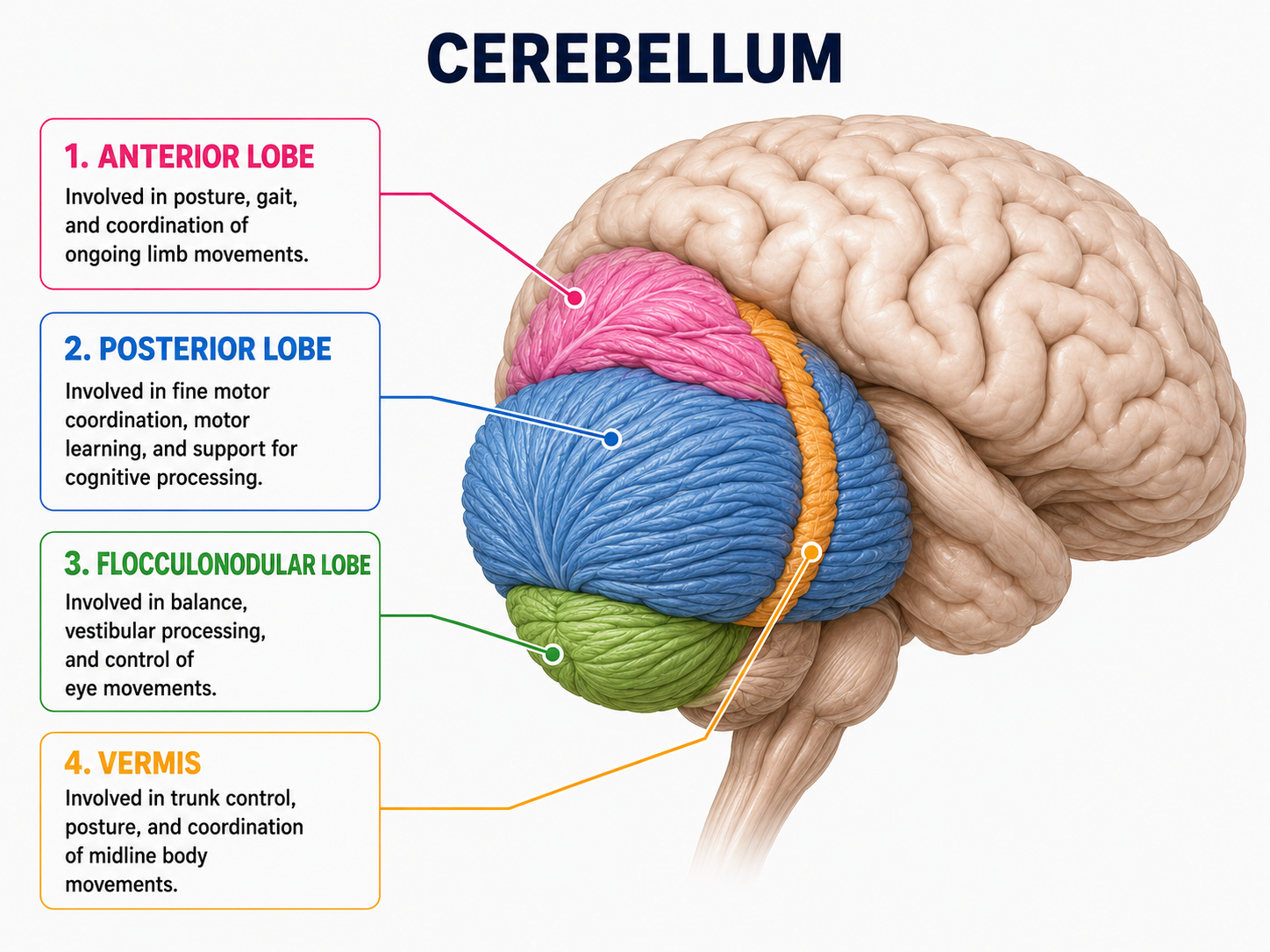
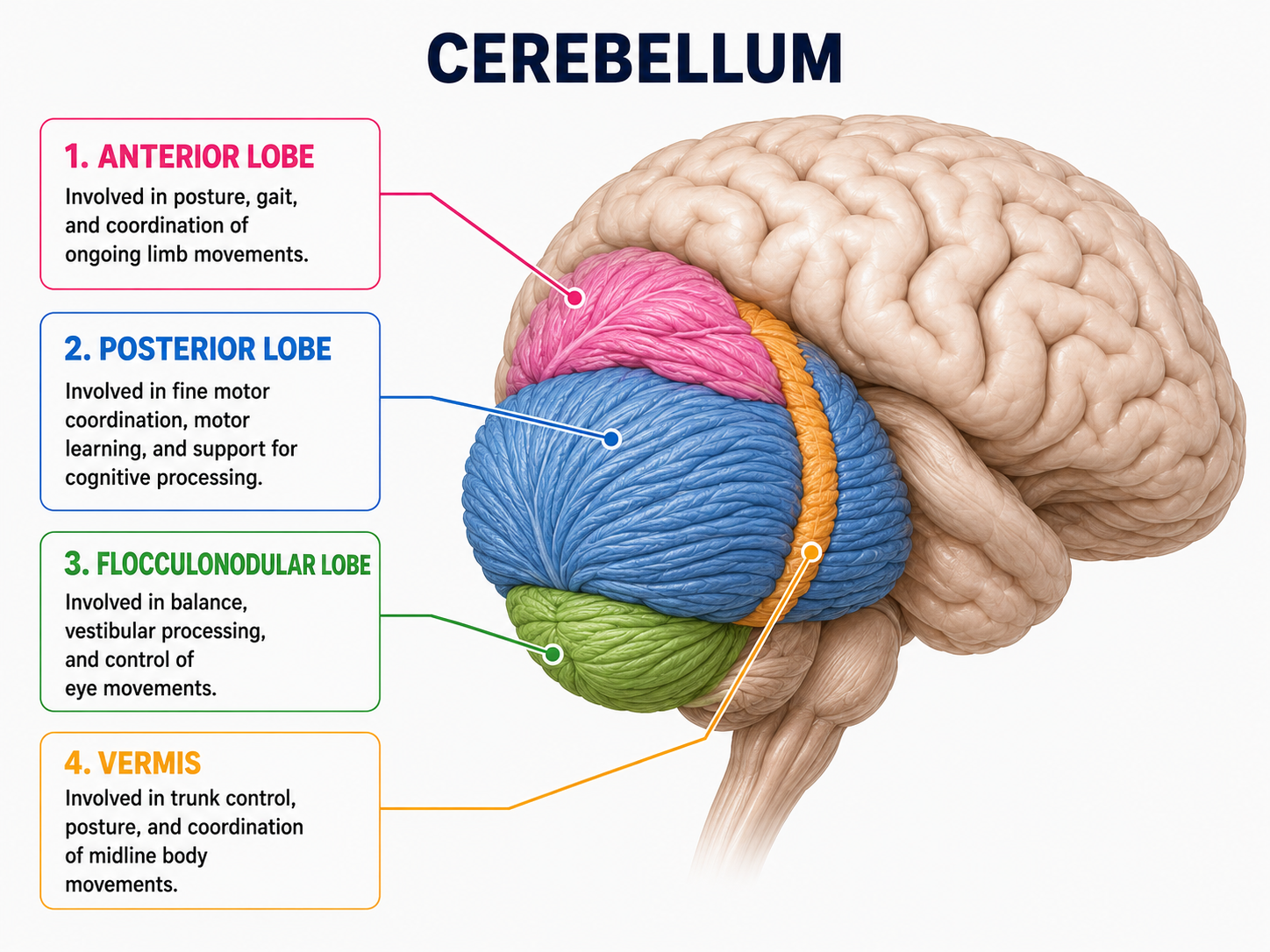
For decades the cerebellum was filed under motor control: coordination, timing, and the smooth execution of movement and posture. That description is not wrong, but it is incomplete. The cerebellum also modulates a wide range of cognitive and affective functions, including language, working memory, spatial processing, executive functioning, and social-emotional regulation.
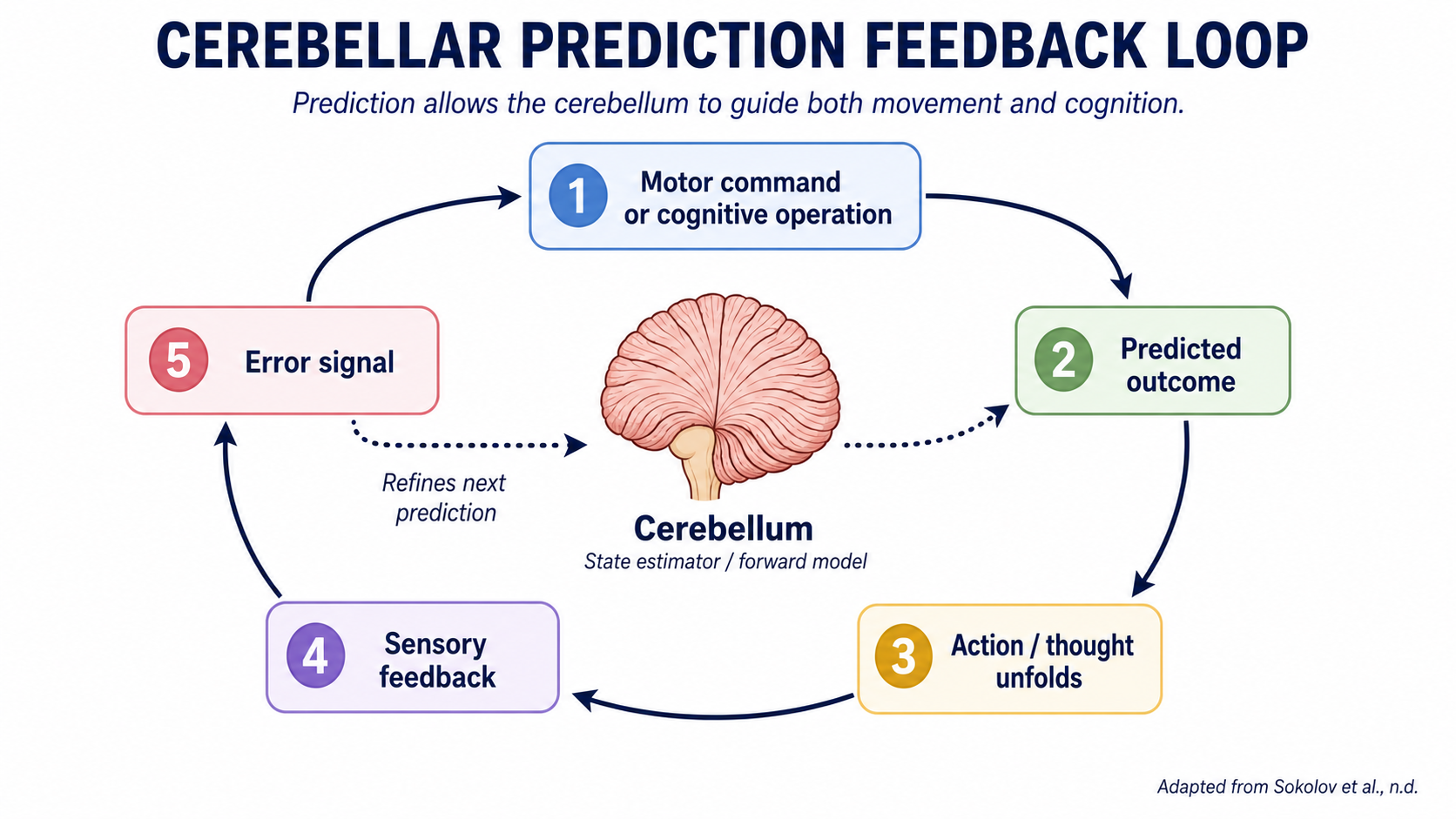
The unifying mechanism behind both roles is prediction. The cerebellum functions as a state estimator, a forward model that predicts the outcome of a motor command or a cognitive operation before feedback arrives, then refines that prediction using error signals from the senses. Computationally, this is close to what engineers call a Kalman filter: a system that continuously weighs an internal prediction against incoming sensory data and blends the two into a corrected estimate, applied here across motor, cognitive, affective, and social domains.
This is why cerebellar patients do not look clumsy in the way a weak muscle looks clumsy. Weakness fails at output. Cerebellar dysfunction fails at prediction.
The movement, the word, the shift in attention, all arrive late and get corrected reactively instead of anticipated smoothly.
Schmahmann (2019) frames this as a loss of the universal cerebellar transform, the automatic, subconscious process that keeps behavior oscillating around a stable baseline across every neurological domain. When that dampening function is disrupted, movement, thought, and mood all lose their smoothness in the same way.
The wiring supports this reach beyond motor cortex. The cerebellum forms a closed loop with the cerebral cortex, receiving input through the pontine nuclei and sending output back through the deep cerebellar nuclei and thalamus (Diedrichsen & McDougle, 2026). The posterior cerebellum connects heavily to prefrontal, posterior parietal, superior temporal, and limbic cortices, the association areas responsible for complex cognition and emotion, while the anterior cerebellum stays tied to spinal, brainstem, and sensorimotor circuits. It also runs disynaptic loops with the basal ganglia, placing it inside the same subcortical network that supports adaptive, goal-directed behavior .
Take Action
You are not testing strength or range. You are testing prediction under uncertainty: can the patient anticipate the outcome of a movement or a mental operation before feedback confirms it, and correct efficiently when the prediction is wrong.
The Setup:
Give the patient a target that changes position or timing just slightly, something they cannot fully anticipate from a static plan. A reach to a cup that gets nudged. A verbal sequencing task where the next item is only revealed at the last second. A weight shift onto a surface with a small, unpredictable give.
Watch for the signature pattern: initial overcorrection, a lag before the correction begins, then a second correction in the opposite direction. That oscillation is the visible signature of a degraded forward model, not a strength or comprehension deficit.

How to Treat This (Real Sessions)
Member Resource: Print out the following information for your quick reference in the clinic!
Perturbation-based training grounded in cerebellar forward-model function:
-
Because the cerebellum generates predictions through active error correction rather than passive repetition, static or fully memorized tasks do not train the system. Unpredictable, self-corrected tasks do.
-
For patients where cerebellar function is partially intact and adaptation is the goal, training needs to involve genuine unpredictability, a target that shifts, a surface that gives, a sequence revealed only at the last moment, not a fixed pattern practiced to automaticity.
-
For patients where cerebellar degeneration is progressive, the goal shifts from rebuilding the prediction loop to reducing the burden on a failing one. Consistent movement patterns, predictable environments, and reduced task complexity lower the demand on a compromised forward model. Slowing the pace of a task and widening the margin for error can partially compensate by giving the delayed feedback loop more time to catch up before the next input arrives.
Cognitive and environmental enrichment as a structural intervention:
-
Environmental and intellectual enrichment is associated with greater cerebellar structural resilience and functional plasticity, framed in the literature as cerebellar cognitive reserve (Van Rossem et al., 2025).
-
This is the same reserve argument made for the cerebral cortex in dementia prevention, but applied to the cerebellum specifically. For patients where cerebellar preservation is a clinical goal, such as early Alzheimer's disease, mild cognitive impairment, or early-stage ataxia, novel and cognitively demanding activity is a structural intervention, not a generic recommendation to stay active.
-
Neuromodulation approaches targeting the cerebellum, including rTMS and tDCS, are being investigated for the same structural and functional goal and may appear on a patient's broader treatment team plan (Van Rossem et al., 2025; Schmahmann, 2010).
Bringing automaticity to conscious awareness:
-
The cerebellum's core contribution is automating multitasking so the cortex is free to do something else. Cerebellar damage strips this out, so a task that used to run in the background now has to be run consciously (Schmahmann, 2010).
-
Every patient with cerebellar involvement on your caseload, regardless of primary diagnosis, needs this addressed explicitly: one task at a time, deliberate attention on the movement or the words instead of divided attention, until the skill either recovers or the patient learns to substitute conscious monitoring for the automatic loop that was lost.
Across Disciplines
PT: Your patient's difficulty with novel gait terrain, stepping over unexpected obstacles, or recovering balance after a small trip is not simply a strength or reaction-time problem. It is a cerebellar forward-model failure that is preventing accurate prediction of the body's next position. Your balance and gait training in unpredictable conditions, uneven surfaces, sudden speed changes, unannounced perturbations, is directly targeting the predictive correction system rather than working around it. Design sessions to include controlled unpredictability early, then progress complexity as corrective oscillations shrink.
SLP: Your patient's delayed word-finding under time pressure, disrupted conversational timing, and difficulty with rapid sequential speech tasks may be cerebellar prediction failures affecting the timing of language production, not isolated word-retrieval or attention deficits. Your cognitive-communication interventions can target timing directly: rapid alternating speech drills, conversational turn-taking with unpredictable prompts, and sequencing tasks where the next item is not known in advance.
OT: Task breakdown failures such as a patient losing the thread of a multistep ADL, needing to stop and consciously re-plan a familiar routine, or struggling when a step in a task is done out of the usual order are signs the automatic sequencing that once ran in the background is gone. Your intervention needs to first reduce the task to single-focus attention, then rebuild sequencing deliberately before reintroducing multitasking demands. Compensation strategies that assume intact automatic sequencing will not generalize. Slow the task down first. Train single-focus execution. Then probe multitasking deliberately.

Documentation
Do not write: "Patient demonstrated poor coordination during reaching task."
Write what actually happened: "Patient demonstrated dysmetria during unplanned reach to shifted target, characterized by initial overshoot followed by delayed corrective adjustment, consistent with impaired predictive motor control. Reduced number of corrective oscillations noted with repeated trials, suggesting early motor adaptation."
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition

Handout 1: Cerebellar Cognitive Affective Syndrome (CCAS) Screening Reference
A one-page reference outlining the domains affected in CCAS, including executive dysfunction, language changes, visuospatial impairment, and affective blunting or disinhibition. Useful for flagging patients whose cognitive presentation does not match a purely cortical injury pattern.
Clinical tip: if a patient's cognitive profile looks scattered across domains rather than clustered in one, check the imaging for cerebellar involvement before assuming a mixed cortical picture.
Handout 2: Perturbation-Based Task Bank Prediction Training
A printable bank of low-equipment activities across OT, PT, and SLP that introduce small, controlled unpredictability into reaching, gait, and language tasks, organized by grading level.
Clinical tip: grade unpredictability, not difficulty. A task that is unpredictable but simple still trains the prediction loop more effectively than a predictable task that is merely harder.
One-Line Clinical Reasoning Starters
Motor Overshoot and Correction | Cerebellar Forward-Model Failure
- Cerebellar forward-model failure identified as the primary mechanism underlying overshoot-and-correct movement pattern
- Patient demonstrates delayed corrective adjustment following unplanned reach, indicating impaired predictive motor control rather than weakness or general incoordination
- Perturbation-based training targeting active prediction and correction indicated to drive adaptation of the degraded forward-model loop
- Corrective oscillation count per trial identified as primary outcome measure across sessions.
Cerebellar Cognitive Affective Syndrome | Scattered Cognitive Profile
- Cerebellar Cognitive Affective Syndrome identified as underlying mechanism for cognitive presentation spanning executive, language, visuospatial, and affective domains
- Cognitive profile inconsistent with an isolated cortical injury pattern; posterior fossa involvement indicated as primary driver
- Skilled cognitive intervention targeting domain-specific deficits indicated rather than generalized cognitive stimulation
- Affective blunting or disinhibition documented as a neurological sequela of cerebellar injury, not a premorbid personality change.
Loss of Automaticity | Conscious Monitoring Required
- Loss of automatic task execution identified as mechanism underlying reduced multitasking capacity following cerebellar injury
- Patient requires deliberate, single-focus attention to complete tasks previously performed automatically
- Compensatory strategy of conscious monitoring indicated as a bridge intervention while automaticity is retrained or substituted
- Multitasking demands to be reintroduced gradually, and only after single-task performance stabilizes.
Balance Plateau on Static Tasks | Perturbation-Based Training Indicated
- Plateau on static balance and stance tasks identified as insufficient challenge to the cerebellar predictive correction system
- Static tasks do not require anticipatory postural adjustment and therefore fail to drive further adaptation
- Perturbation-based balance and gait training indicated to reintroduce prediction demand and resume functional progress
- Corrective response latency and magnitude identified as measurable indicators of continued adaptation.
Cerebellar Cognitive Reserve as a Structural Intervention
- Environmental and cognitive enrichment prescribed as a structural intervention targeting cerebellar volume and functional plasticity preservation in patient with early cognitive decline
- Evidence base supports an association between enrichment and cerebellar structural resilience, paralleling the cognitive reserve argument established for the cerebral cortex
- Enrichment activity documented as a neuroplasticity intervention, not a general lifestyle recommendation
- Novel, cognitively demanding activity prioritized over repetitive or passive activity in session and home program design.
See you in the next newsletter


Responses