

You've seen this patient.
They can follow instructions in a quiet room.
They can move their arm when you cue them.
They can answer your questions.
....But the moment you ask them to sit unsupported and reach at the same time....
👉 everything falls apart.
That's not weakness.
👉 That's cognitive load.
And this activity addresses all of it with two chairs, a piece of tape, three targets.
This is the fourth activity in this series built from materials that cost nothing. Two chairs exist in every clinic, every home, every waiting room. The tape you already have. The cognitive intervention is in how you set it up.
What the activity actually is
Setup:
🪑🪑 Two chairs facing each other
➿ A piece of tape or paper on the back chair as a target surface
Three tiers: one target below midline, one at neutral, one above shoulder height — Patient seated on the front chair, hands in hand-under-hand position on the back chair
The task: patient reaches forward and down to the bottom target, returns to midline, reaches to the middle target, returns, reaches to the top target, returns.
That is one sequence.
Grading Ideas
👉 Grade by pushing the front chair forward — more distance means more trunk load.
👉 Grade by moving from supported sit to unsupported sit.
👉 Grade by adding trunk rotation — place targets in a corner so the patient must rotate to reach both sides.
👉 Grade by adding weight to the bar for progressive resistance.
Three tiers. Infinite progressions.
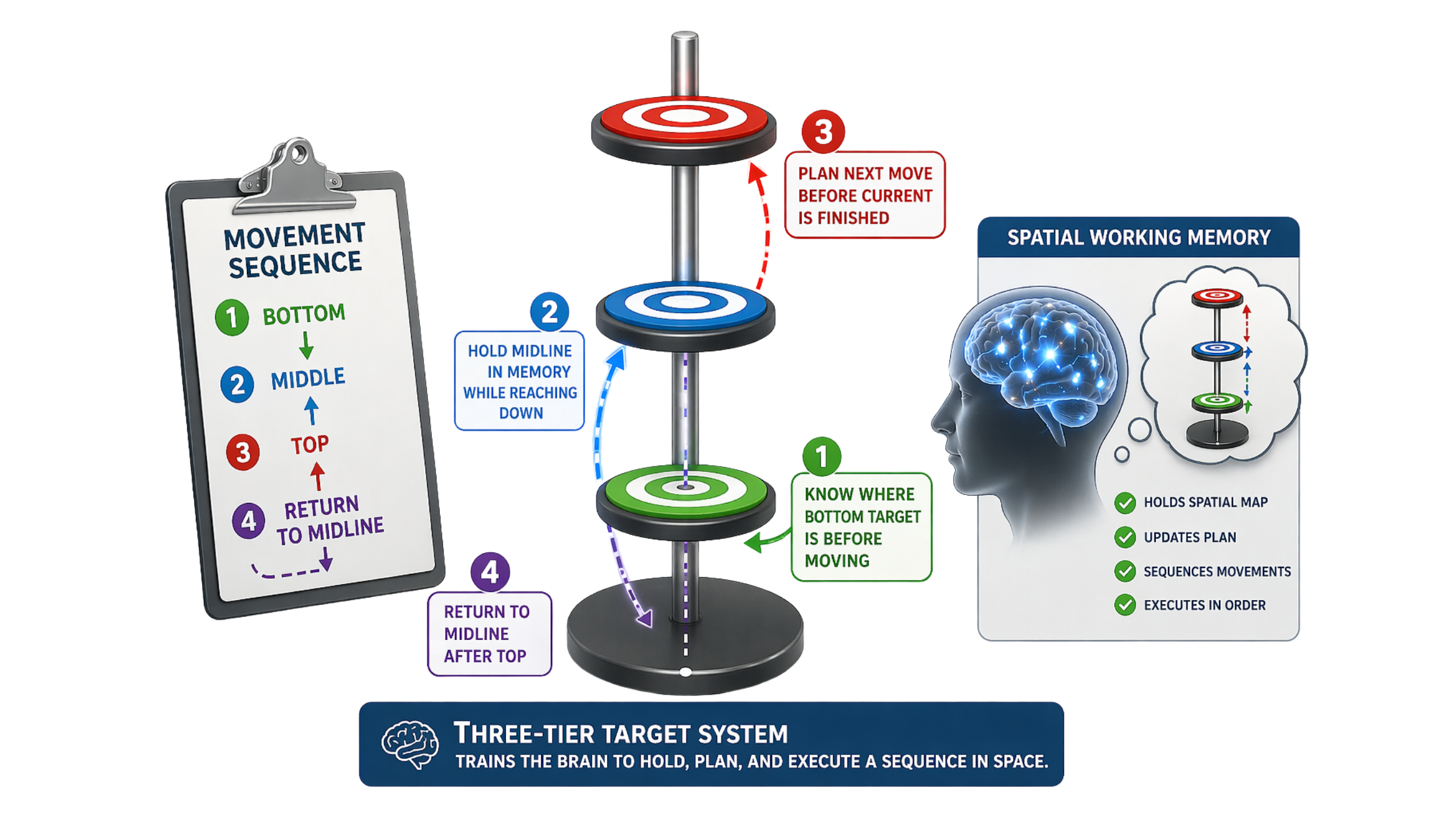
Why this is a spatial working memory intervention
Before the patient reaches to the bottom target —
👉 their brain has to know where the bottom target is.
Before they return to midline —
👉 their brain has to hold the midline location in working memory while executing the downward reach.
Before they move to the middle tier —
👉 their brain has to plan the next movement before the current one is finished.
That is anticipatory motor planning.
The three-tier target system forces the brain to hold a spatial map of the movement sequence — bottom, middle, top, return — and execute each element in order without losing the plan.
This is spatial working memory.
The same cognitive process that allows your patient to navigate their kitchen without bumping into things. To plan a transfer before they stand. To reach for an object on a shelf without knocking over what's next to it.
👉 The three targets are not just reach destinations.
👉 They are a spatial working memory protocol embedded in a seated activity.
When the patient loses their place in the sequence — reaches to the wrong tier, skips a target, needs repeated verbal cuing — that is not inattention.
👉 That is spatial working memory failure.
Document it as such.
Why this is a postural cognitive load intervention
Supported sitting is baseline.
The moment you remove the support — push the chair back, take away bilateral upper extremity weight-bearing — you have added a postural cognitive demand to every single movement.
Now the patient is simultaneously:
— Maintaining trunk alignment without support
— Planning and executing the reach sequence
— Holding the spatial map of the three tiers
— Monitoring the affected upper extremity through the unaffected hand
👉 That is a full dual-task postural-cognitive intervention.
The dual tasking cost framework applies here directly. If the patient's reach accuracy deteriorates when bilateral UE support is removed — if they start losing their place in the sequence, skipping tiers, or reaching off-target — you have identified the postural cognitive load ceiling.
👉 That is a functional safety finding.
A patient who cannot maintain spatial working memory for a three-tier reach sequence under postural demand is a patient who is at risk during any real-world activity that requires simultaneous trunk control and motor planning — transfers, bed mobility, reaching in the kitchen, getting dressed.
Document the ceiling. Grade to it systematically. That is skilled clinical reasoning.
Why this is a motor initiation intervention
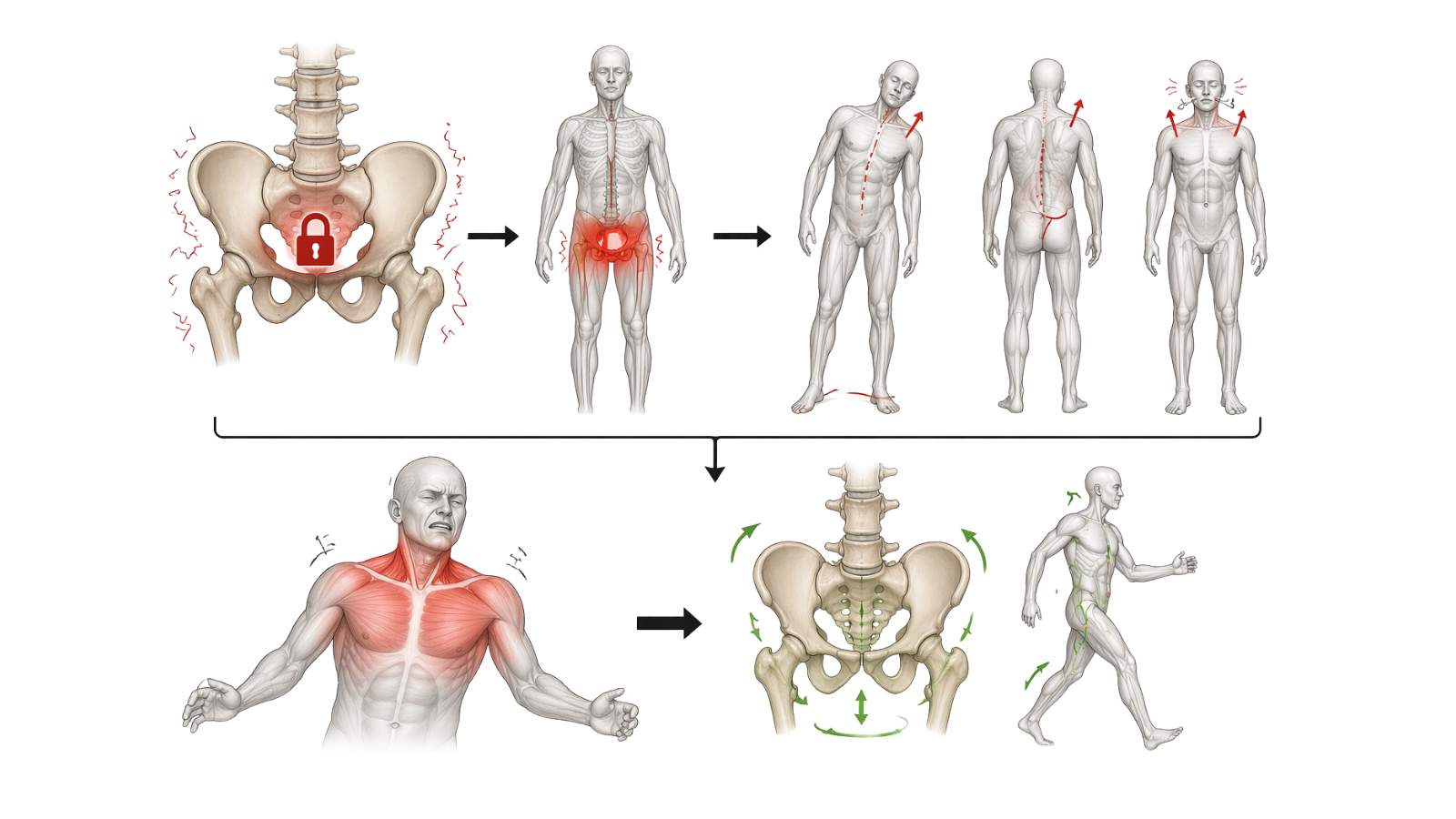
The pelvis is stuck.
👉 This is one of the most common and undertreated findings in neurological rehab.
Whether the cause is hemiplegia, chronic pain, deconditioning, or prolonged bed rest — a pelvis that cannot move freely is a pelvis that cannot support dynamic trunk movement superimposed on it. The patient compensates with their upper body. They hike their shoulder. They lean to one side. They hold their breath.
👉 None of that is a strength problem.
👉 All of that is a motor initiation problem.
The forward reach in this activity (especially when the chair is pushed forward to increase the load) forces pelvic anterior tilt and trunk flexion.
The return to midline requires the pelvis to actively participate in the movement rather than remain passive.
When you cue the patient to visualize their scapulas folding around their ribcage and their pelvis tilting forward, you are asking the brain to generate a motor command it has stopped generating automatically.
That is motor initiation.
The same executive function process that allows your patient to initiate getting out of bed in the morning, stand up from a chair without five verbal cues, or begin a task without being repeatedly prompted.
When the pelvis begins to move (when you see that forward tilt, that trunk flexion, that scapular protraction) that is not just mobility.
👉 That is the executive function system re-engaging with the motor system.
Document it as a skilled clinical outcome.

How to Treat This (Real Sessions)
🪑 Start with hand-under-hand, not hand-holding. The unaffected hand cradles the affected hand from underneath. This recruits the unaffected side as an active monitor — the palm cup provides proprioceptive feedback to the affected limb throughout the reach. Hand-on-top does not do this. Hand-under-hand does.
📍 Set all three tiers before the session starts. Don't adjust targets mid-session. The patient needs to build a consistent spatial map of the target locations. Changing them resets the working memory demand and disrupts motor learning. Make changes between sessions, not during them.
📏 Measure and document the chair distance. The distance between the front leg of the patient's chair and the front leg of the back chair is your objective postural load measure. Record it every session. Increasing the distance is a progression variable — treat it like weight on a barbell.
🪞 Use the mirror for alignment, not for encouragement. Place it directly in front of the patient so they can self-monitor shoulder hiking, trunk lean, and midline position. Visual biofeedback during movement is a motor learning strategy — not a reassurance tool. Tell the patient what to look for before the movement begins.
🔄 Add trunk rotation last. Place targets in a corner setup — one on each wall — only after the sagittal plane sequence is clean and consistent. Trunk rotation adds a full axial movement demand to the spatial working memory load. It is a significant progression, not a variation.
⬆️ Grade the support removal one variable at a time. Supported sit first. Then reduce bilateral UE support by pushing the chair forward. Then remove the chair entirely and move to unsupported sit. Never remove support and increase chair distance in the same session.
Across Disciplines (Same System, Different Look)
This is OT-led — but the principles apply everywhere.
PT: dynamic sitting balance under concurrent reach demand is a dual-task postural-cognitive intervention by definition. The three-tier target system introduces the same spatial working memory demands present during functional mobility (e.g., bed mobility sequencing, transfer planning, stair navigation). The chair-distance progression is a measurable postural load variable. Use it as one.
SLP: motor initiation deficits (i.e., the frozen pelvis, the inability to begin a movement without repeated cueing) map directly onto initiation deficits in communication. A patient who cannot initiate a trunk movement without three verbal prompts is often the same patient who cannot initiate a spoken response without prompting. Same prefrontal system. Different output channel.
👉 One activity. One cognitive system. Three different functional presentations.
Documentation
🧠 Document the system, not just the movement.
This is not just a reaching task.
Identify and document the cognitive systems involved:
— spatial working memory (multi-tier sequencing)
— postural cognitive load (trunk control under demand)
— motor initiation (pelvic and trunk activation)
👉 If you don’t name it, it doesn’t exist clinically.
📍 Describe where the breakdown occurs.
Don’t write “patient required cues.”
Write what actually happened:
— lost sequence between tiers
— reached to incorrect target
— paused mid-task with loss of plan
— required cueing to re-initiate movement
👉 This is spatial working memory breakdown—not inattention.
📏 Measure the postural load.
The distance between chairs is not setup—it’s data.
Document:
- chair-to-chair distance
- level of UE support (bilateral, unilateral, none)
- sitting condition (supported vs unsupported)
👉 Increased distance = increased cognitive-postural demand.
Track it across sessions.
⚖️ Document the dual-task cost.
When support is reduced:
- does accuracy decrease?
- does sequencing break down?
- does movement become less controlled?
👉 This is the postural cognitive load ceiling.
This is a functional safety finding.
🔄 Capture motor initiation changes.
Watch the pelvis—not just the arm.
Document:
- presence or absence of anterior pelvic tilt
- trunk flexion vs compensatory shoulder movement
- delay in movement initiation
- reduction in verbal cueing required
👉 Improved pelvic activation = improved motor initiation.
This is a skilled outcome.
📊 Track functional cognitive outcomes.
Not just reps.
Measure:
- number of sequences completed correctly
- number of cues required
- accuracy across all three tiers
- ability to maintain sequence under increased demand
👉 This reflects cognitive-motor performance—not strength.
🧾 Tie it to function.
Make the connection explicit:
- transfers
- reaching during ADLs
- task sequencing
- safety during dynamic movement
👉 This is not exercise.
👉 This is functional performance training.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!
What's included:
- Handout 1: Pelvic Positioning — Executive Function Reference — the full pelvic anatomy and positioning guide for identifying, observing, and documenting pelvic findings as motor initiation and postural cognitive load targets
- Handout 2: Standing Balance and Posture — your clinical progression framework from static to dynamic standing, with the body activation continuum, dual-task layering protocol, and cross-disciplinary documentation language
- Clinical application guide below — how to use each resource to sequence evaluation, grade the postural-cognitive demand, and document findings that justify skilled intervention
Handout 1 — Pelvic Positioning: Executive Function Reference
This is your observation and documentation anchor. Before you place the patient in any seated activity — including the three-tier reach you just read — identify pelvic position at rest and during movement initiation. The four positions (anterior tilt, posterior tilt, neutral, lateral obliquity) are not just postural findings. Each one tells you something specific about what the trunk can and cannot do during functional activity.
Best used for: Identifying baseline pelvic position before the session begins, documenting compensation patterns during forward reach, connecting pelvic mobility findings to motor initiation as an executive function target — not just a mobility deficit.
Clinical tip: Use the clinical observation guide on page 3 in real time during the reach activity. You are watching three moments: baseline position before movement, anterior pelvic tilt during forward reach, and active vs. passive return to midline. A pelvis that moves forward but cannot actively return is a different clinical finding than one that never moves at all. Document both separately. They require different interventions and they tell different stories about where the motor initiation breakdown is occurring.
Pelvic Mobility - Executive Function Reference Packet
Handout 2: Standing Balance and Posture: Clinical Progression Framework
This is your sequencing and grading reference. The framework moves from static sitting balance through dynamic standing, with the body activation continuum as the load progression structure. Every level has a dual-task layer — and the rule is consistent across all four levels: the motor component must be clean for three or more consecutive reps before any cognitive demand is introduced.
Best used for: Determining where in the progression your patient currently is, grading postural-cognitive load systematically across sessions, and generating documentation language that reflects functional safety findings — not just motor performance.
Clinical tip: The dual-task cost is your outcome measure, not the motor task itself. A patient who can complete Level 2 stepping cleanly but loses postural alignment within two reps when a verbal task is introduced has given you a specific, documentable functional safety finding. That is not a motivational issue. That is a postural cognitive load ceiling. Name it, measure it session to session, and use it to justify continued skilled care. The framework gives you the language — use it exactly as written in your notes.
Standing Balance and Posture Resource
Clinical Application Guide: Connecting Both Handouts to the Three-Tier Reach
Before the session — establish the pelvic baseline
Pull Handout 1. Before the patient touches the chair, observe pelvic position at rest. Posterior tilt at baseline means reduced trunk mobility before the activity even begins — document it as your starting condition, not as a barrier. Use the four-position reference to name exactly what you see. This takes thirty seconds and gives you the clinical anchor for everything that follows.
During the reach — observe in the sequence the guide gives you
Use the three-column observation framework on page 3 of Handout 1: baseline, during forward reach, return to midline. You are not watching the arm. You are watching whether anterior pelvic tilt initiates before shoulder movement, whether the trunk flexes or the shoulder compensates, and whether the return to midline is active or passive. That sequence is your motor initiation data.
When the patient is ready to stand — use Handout 2 to determine entry point
Do not move to standing until sitting balance — static, then dynamic — is established. Handout 2 gives you the sequencing rule and the clinical rationale for it. When the patient is ready, enter the body activation continuum at the appropriate level based on what you observed in the seated activity. The postural findings from Handout 1 tell you which level to start at. A patient with persistent posterior tilt, absent anterior pelvic tilt during reach, and compensatory shoulder hiking is not yet a Level 2 candidate.
Grading across sessions — treat both handouts as one system
Pelvic mobility is the foundation. Standing balance is the load. Use Handout 1 to track whether cue count to generate anterior pelvic tilt decreases session to session — that is your motor initiation outcome variable. Use Handout 2 to track at which body activation level dual-task cost appears — that is your postural-cognitive load ceiling. When the ceiling rises, that is your evidence of functional improvement. Document both in every session note.
Documentation Language
✏️ Name the deficit: Patient demonstrated absent anterior pelvic tilt during forward reach with compensatory shoulder hiking bilaterally; posterior pelvic tilt at rest limiting dynamic trunk mobility as a foundation for upper extremity function and standing balance progression.
🔗 Link to function: Pelvic mobility deficits and postural cognitive load ceiling impacted safe performance of transfers, seated ADL tasks, and any activity requiring concurrent trunk control and upper extremity engagement.
🔥 Skilled intervention: Clinician implemented graded seated reach activity with systematic postural observation per pelvic positioning framework, progressive chair distance advancement, and real-time motor initiation facilitation targeting anterior pelvic tilt, trunk flexion, and return to midline.
⚕️ Medical necessity: Skilled intervention required to identify motor initiation versus strength deficit, sequence postural-cognitive load grading from seated to standing, and facilitate executive function re-engagement with the motor system — clinical judgment required at each progression point to advance demand safely without postural collapse.
One-Line Clinical Reasoning Starters
- Absent anterior pelvic tilt during forward reach reflects motor initiation failure — not weakness — and requires skilled neuromuscular facilitation to restore prefrontal engagement with the motor system.
- Posterior pelvic tilt at rest is a trunk mobility baseline deficit that limits dynamic reach, transfer safety, and standing balance progression — skilled evaluation and grading are required before any standing intervention is introduced.
- Postural cognitive load ceiling identified during dynamic standing with concurrent verbal task — functional safety implications extend beyond isolated balance findings and require skilled dual-task grading.
- Reduction in verbal cues required to generate anterior pelvic tilt is a measurable motor initiation outcome — track cue count per session as your primary functional variable.
- Static-to-dynamic standing progression requires skilled real-time judgment to sequence postural load, dual-task demand, and BOS reduction — cannot be replicated through unskilled instruction or unsupervised home exercise at this stage.

Responses