

This activity looks like hand therapy.
It's actually a cognitive intervention.
The most important part of your session isn't what happens in the clinic.
It's what happens when you leave the room.
If your patient can only perform a task with your equipment, in your clinic, with you present —
👉 they haven't learned anything yet.
👉 the motor map is still clinic-dependent.
👉 generalization has not occurred.
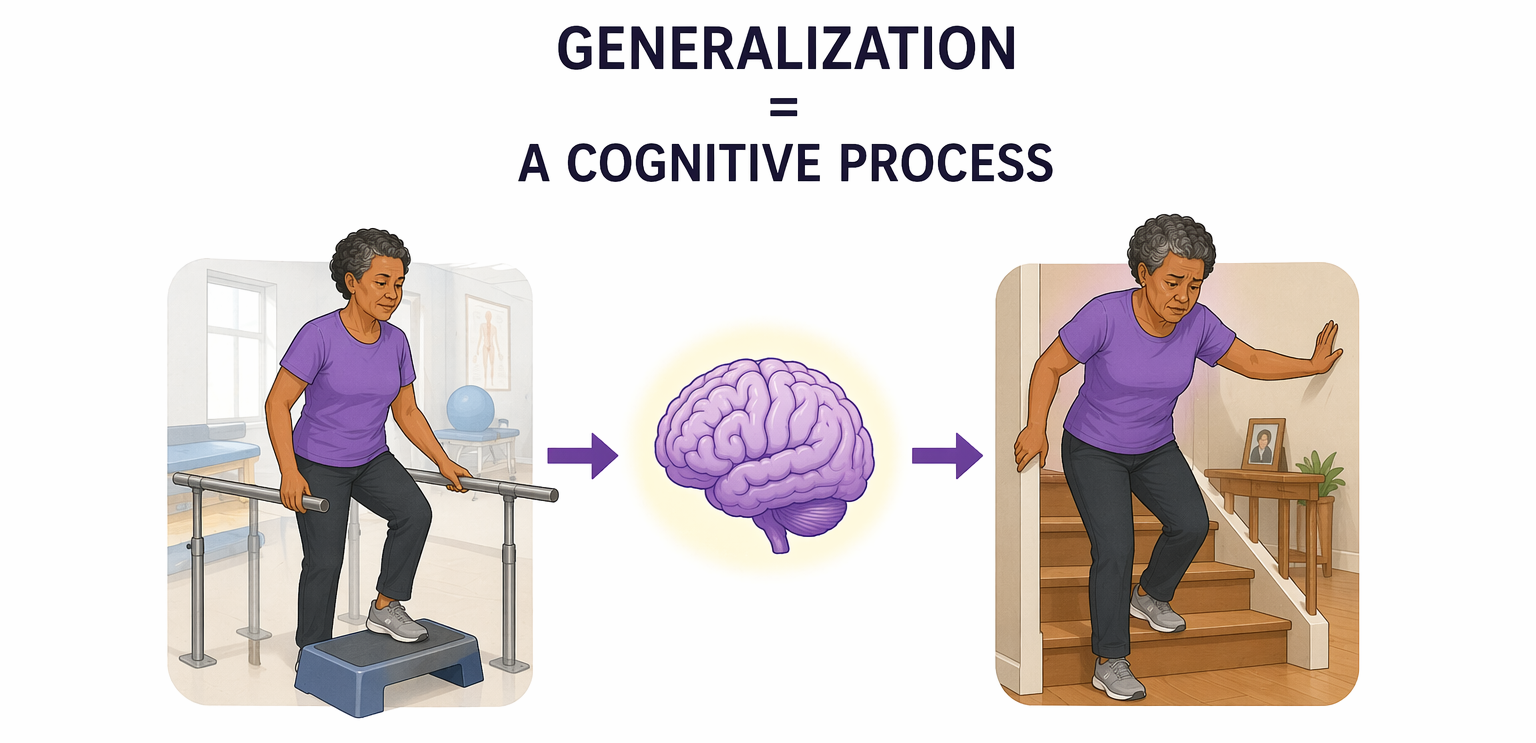
And here's what most clinicians don't realize:
👉 Generalization is a cognitive process.
The brain doesn't automatically transfer a skill from one environment to another. It has to build a map that is flexible enough — and context-independent enough — to travel. The more complex the equipment required to perform the task, the higher the cognitive load of that transfer. And the higher the cognitive load, the more likely it fails.
This is not a theory.
👉 This is why your patient does it perfectly in the clinic and falls apart at home.
What this activity actually is
Everything you need:
— A roll of masking tape (~$2, available anywhere) — A table — The patient's hand
Set five tape targets on the table surface, spaced roughly to match the patient's finger width. Number them 1 through 5. That's it.
The task: active range of motion — digit taps, flexion, extension, abduction, adduction, isometric presses — using the numbered targets as visual anchors.
👉 That's it.
👉 Except it's not simple at all.
Why this is a generalization intervention first
The minimalist philosophy is not about being basic.
👉 It is about being neurologically sound.
When you use masking tape and a table, you are using materials your patient has access to everywhere — at home, at work, at their kitchen table, in a hotel room, at their grandchild's house. The motor map they build in your clinic with these tools is a motor map they can access in every one of those environments without modification.
When you use specialized equipment, you create a context-dependent map.
🧠 The brain learns: I do this here, with this tool, in this room.
When you use a piece of tape and a surface:
🧠The brain learns: I do this anywhere, with anything, at any table.
That is not the same skill. And the difference between those two is entirely cognitive.
Progressive overload — the principle that drives motor learning — requires consistency with the same muscle groups and the same movement demands. Variety of tools disrupts the map. Consistent tools with graded demand builds it.
👉 You are not being basic.
👉 You are building a transferable skill.
Why this is an attention intervention
Masking tape targets are external cognitive supports.
When a patient has difficulty with isolated digit control, their attention system is working hard to suppress the wrong fingers while activating the right one. The tape target gives the attention system something to anchor to — a visual reference that reduces the cognitive load of spatial accuracy so the motor system can focus on the movement itself.
This is the same principle as written cue cards for verbal instructions.
👉 Reduce the cognitive load on one channel so the other can do its job.
The metronome takes this further. For neurological patients, tapping to an external rhythm adds a reaction time demand — the brain has to match motor output to an external temporal cue. This directly targets information processing speed.
👉 You built an IPS intervention out of a metronome and a piece of tape.
Why this is a dual tasking intervention
Number the targets.
Give a sequence: 5, 3, 1, 4, 2.
Now ask the patient to tap in that order while maintaining isolated digit control and postural alignment.
👉 Motor demand: isolated joint activation, controlled flexion and extension, sustained isometric hold
👉 Cognitive demand: working memory for the sequence, selective attention to the correct target, inhibition of the wrong fingers
That is a full dual-task cognitive intervention.
You can start with one tap and build to sequences of 10 or more. You can run forward and backward. You can add the metronome as a third layer. You can use bilateral simultaneous engagement for patients with neurological deficits — both hands tapping in sequence, coordinating across midline.
👉 One roll of tape. One table.
👉 Attention, working memory, processing speed, motor learning, and generalization — all in one session.

How to Treat This (Real Sessions)
🧩 Start without numbers. Run digit taps, abduction/adduction, and flexion/extension without any sequencing first. Establish the motor baseline before adding the cognitive layer.
📍 Position the targets for the patient, not the protocol. Adjust the tape spacing to match the patient's actual finger width. Sloppy setup means sloppy movement — the targets are only useful if they're accurate.
🎵 Add the metronome before you add the numbers. Rhythm is a lower cognitive load than sequence. Get the patient tapping to an external beat before asking them to hold a number order in working memory. Try this GOOGLE Metranome to get you started!
🔢 Grade the sequence, not just the movement. One number. Then two. Then three. Document the highest sequence length the patient can execute with accurate digit isolation. That's your functional cognitive measure.
💪 Use isometric presses as a reset between sets. Push down for five seconds, release. This is not just strengthening — it is a sustained attention and body awareness task. Include therapist-initiated rest between sets and document it.
🏠 Send it home on day one. Give the patient a piece of tape and a written number sequence before they leave. The whole point is that they can do this anywhere. If you don't give them the home program, you undermine the generalization rationale entirely.
Across Disciplines (Same System, Different Look)
This is OT-led — but the principles apply everywhere.
PT: any fine motor or isolated joint activity that adds a sequencing or timing demand is running the same cognitive load. Numbered targets on a therapy surface are as applicable to lower extremity isolation work as to hand therapy.
SLP: digit isolation taps to a metronome require the same temporal processing and reaction time as phoneme-level speech tasks. The external rhythm principle — using a metronome to anchor motor output — is directly applicable to rate and rhythm work in dysarthria treatment.
👉 Same cognitive system. Different functional presentation.
Documentation
✏️ Name the defecits:
Patient demonstrated decreased isolated digit control with compensatory mass finger activation, limiting fine motor task performance and functional hand use.
Link the function:
Deficits impacted ability to perform tasks requiring isolated finger movements including writing, buttoning, medication management, and device use.
Skilled intervention:
Clinician implemented graded active range of motion protocol with visual target anchoring and progressive dual-task sequencing demands targeting motor learning, sustained attention, working memory, and information processing speed.
Medical necessity:
Skilled intervention required to grade cognitive-motor dual-task demands, establish home generalization program, and progress sequencing complexity — clinical judgment required to advance task demands safely and effectively.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition

Member Resource: AROM & Cognitive Dual Tasking Clinical Pack
What's included:
- Handout 1: Classification of Human Hand Movements — the full osteokinematic movement reference guide
- Handout 2: Graded Tap Sequence Bank — 10 levels of cognitive-motor dual tasking with bilateral sequences, metronome guide, and session documentation framework
- Clinical application guide below — how to use each resource to set up, grade, and document the masking tape AROM activity
Handout 1 — Classification of Hand Movements
This is your movement grading reference. Before you set up the masking tape targets, identify which osteokinematic movements your patient currently has — and which ones you are working toward. The activity in this newsletter can be adapted for any movement pattern on this chart: abduction and adduction for digit spreading, flexion and extension for digit isolation taps, pronation and supination as a warm-up before adding the cognitive layer, wrist flexion and extension for patients who need to address wrist mobility alongside fine motor control.
Best used for: Identifying the available movement repertoire before the session, documenting the specific movements being trained, explaining to patients and families exactly what you are working on and why it matters for their daily hand use.
Clinical tip: Before introducing any numbered tap sequence, run through the movement chart with your patient. Identify which movements are available, which are limited, and which are compensatory. The tap sequence you assign should only use movements the patient can currently execute with some degree of isolation — not movements they are still learning. The cognitive layer only works if the motor foundation is there to support it.
Osteokinematic Movement Resource
Handout 2: Graded Tap Sequence Bank
This is your full cognitive-motor progression resource for the masking tape activity. It contains 10 levels of graded tap sequences organized by cognitive demand, a bilateral sequence section, a metronome tempo guide, and a session documentation framework.
Level 1 — Single Tap Isolation: No metronome. This is your baseline. If your patient cannot isolate a single digit without mass finger activation, start here regardless of their overall functional level. Use the movement chart from Handout 1 to confirm which digits have isolated voluntary control before assigning any sequence.
Levels 2–5 — Patterned and random sequences: This is where the dual-task intervention lives. Patterned sequences first — the brain can anticipate. Random sequences second — the brain must hold the instruction in working memory without a predictive scaffold. Add the metronome only after the patient is accurate at the sequence level without tempo. Never introduce tempo and a new sequence level on the same day.
Level 3 — Repeat from memory: The first level that introduces consolidation demand. The patient must retrieve the sequence repeatedly without being re-cued. This is where you will first see the difference between attention failure and working memory failure. Document which one you are seeing — they require different treatment targets.
Levels 6–10 — Extended sequences: Sustained attention and cognitive-motor fatigue become clinical variables. Monitor for digit isolation quality deteriorating before sequence accuracy deteriorates — that is the first sign of cognitive-motor fatigue and a documentable functional finding.
Bilateral sequences: Use when the patient has neurological deficits requiring bilateral coordination, or when the unilateral task has plateaued and you need to increase cognitive demand without increasing sequence complexity. Asymmetric alternating bilateral sequences — two independent sequences executed in alternating order — are the highest cognitive demand in the bank.
Best used for: Establishing a baseline cognitive-motor level, grading the dual-task layer systematically across sessions, progressing from single-channel motor practice to full bilateral cognitive-motor demands, and generating a quantifiable cognitive measure for documentation.
Clinical tip: The session documentation framework at the end of Handout 2 is your clinical measure. Record the highest level achieved with accurate isolated digit activation, the metronome tempo, the sequence type, and the error pattern. "Patient demonstrated working memory capacity for 4-tap random sequences with accurate digit isolation at 50 BPM" is a skilled functional cognitive finding — not just a motor observation. Use it.
Clinical Application Guide: Matching the Breakdown to Your Treatment
Before the session — establish the movement baseline
Pull Handout 1. Run through the available osteokinematic movements with the patient. Confirm which digits have isolated voluntary control. Do not assign a tap sequence that uses movements the patient cannot yet isolate. This is not assessment — it is clinical prerequisite screening. Document it as such.
Setting up the targets — position for the patient, not the protocol
Place five masking tape targets on the table surface. Adjust spacing to match the patient's actual finger width. Number them 1 through 5. If you are targeting visual scanning or hemispatial neglect, spread targets across the affected side or across the full surface. If you are starting with pure motor isolation, keep them close and centered.
Introducing the cognitive layer — sequence before tempo
Start at Level 1 with no metronome. Establish accurate digit isolation across all five targets. Then introduce a Level 2 patterned sequence — still no metronome. Add metronome only after accuracy at the sequence level is established. When you do add tempo, start at 40–50 BPM regardless of the patient's apparent functional level. Do not skip this step.
Grading up — use the level framework
Advance one variable at a time: sequence complexity, sequence type (patterned to random), or tempo. Never advance two variables simultaneously. Use the three-consecutive-accurate-sequences criterion from Handout 2 as your progression gate. If the patient fails, identify whether the error is in sequence recall, digit isolation, or tempo — each requires a different clinical response.
Sending it home
Give the patient a piece of tape and a written sequence before they leave. Write the sequence on a card: their current level, their target digits, and their tempo if using a metronome app at home. The generalization argument only holds if you actually send the home program. Document that you did.
Documentation Language
✏️ Name the deficit: Patient demonstrated decreased isolated digit control with compensatory mass finger activation and impaired working memory for motor sequencing demands, limiting fine motor task performance and functional hand use.
🔗 Link to function: Deficits impacted ability to perform tasks requiring isolated finger movements including writing, buttoning, medication management, and device use.
🔥 Skilled intervention: Clinician established osteokinematic movement baseline using movement classification reference, implemented graded active range of motion protocol with visual target anchoring and progressive dual-task sequencing demands, and assigned context-independent home program to support generalization.
⚕️ Medical necessity: Skilled intervention required to grade cognitive-motor dual-task demands, establish isolated digit control baseline, and progress sequencing complexity — clinical judgment required to advance task demands safely and ensure appropriate home program design for generalization.
One-Line Clinical Reasoning Starters
Use these when documenting medical necessity or justifying continued skilled care:
- Generalization of fine motor skills requires context-independent motor map development — use of clinic-specific equipment limits transfer to home and community environments.
- Digit isolation under dual-task sequencing demand reflects real-world functional requirements for activities including writing, device use, and meal preparation.
- Progressive sequencing complexity requires skilled judgment to advance cognitive load appropriately without exceeding the patient's working memory capacity.
- External rhythm cueing via metronome addresses information processing speed deficits directly impacting reaction time and motor coordination for functional task performance.
- Cognitive-motor fatigue monitoring during extended sequences requires skilled real-time clinical observation — deterioration of digit isolation quality precedes sequence accuracy failure and cannot be identified through unskilled observation.


Responses