

This activity looks like hand therapy.
It's actually a cognitive intervention.
You've seen the power web in the clinic.
Maybe you've used it for grip strengthening.
Maybe for fine motor coordination.
👉 But here's what most clinicians miss:
👉 When you use it for tone inhibition and movement reintegration — you are running one of the most cognitively demanding interventions in your toolkit.
Motor learning. Intentional movement control. Dual tasking.
👉 All three. At the same time.
What the activity actually is
Setup is simple and cheap.
— A resistive power web (~$30) — Pipe connectors from a hardware store (~$8 for a pack) — Bingo disks or paper circles from the dollar store
Insert the pipe connectors throughout the web. Spread the targets across the surface. If your patient has hemispatial neglect, load that side. If you're targeting visual scanning or gaze shifting, spread them everywhere. If you want a cognitive layer, assign a color sequence — red first, blue second, green third.
The task: patient uses the affected upper extremity to pull a connector from the resistive web, reach to a target, place the connector over it, and release.
👉 That's it.
👉 Except it's not simple at all.
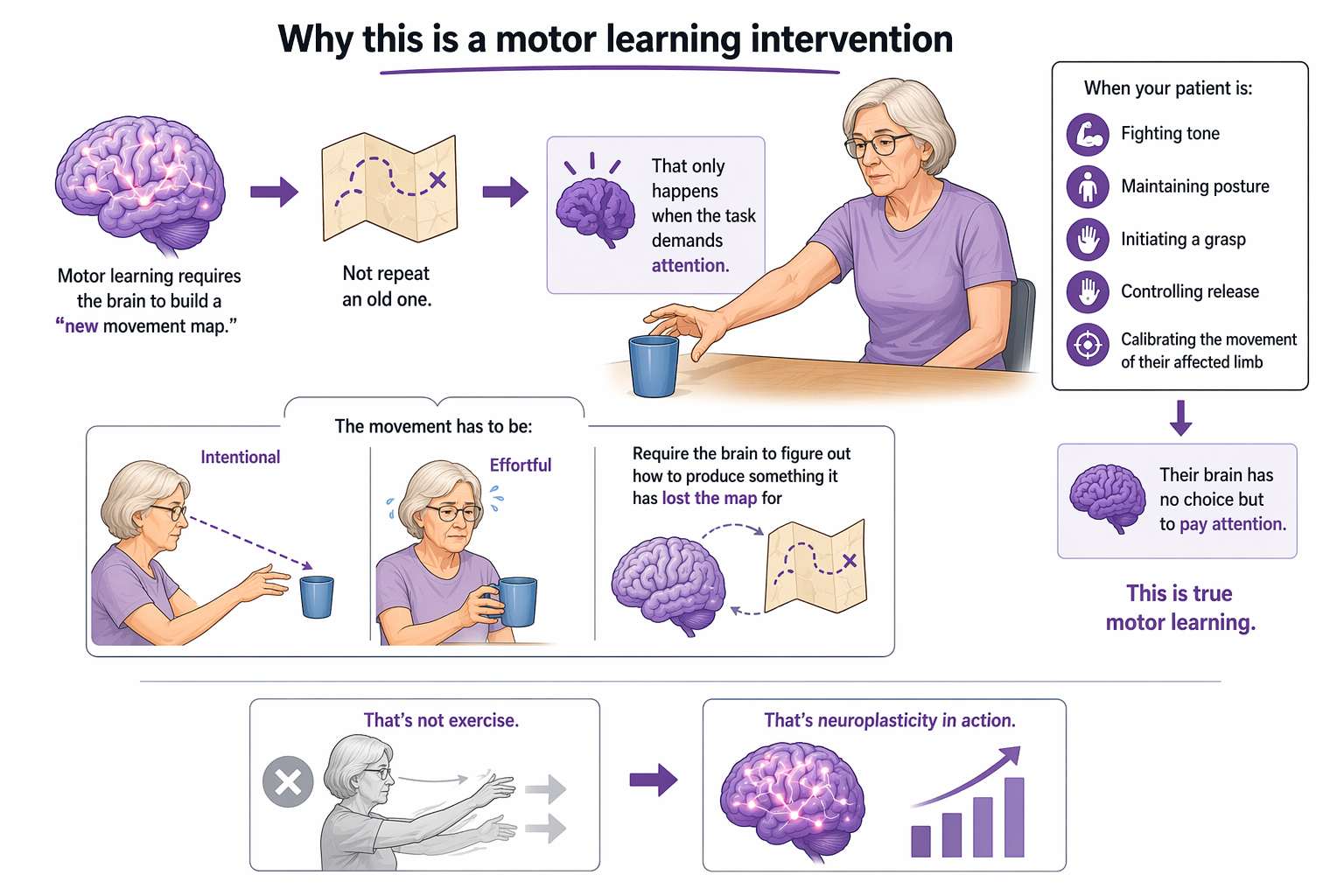
Why this is a motor learning intervention
Motor learning requires the brain to build a new movement map.
Not repeat an old one.
👉 That only happens when the task demands attention.
When your patient is fighting tone, maintaining posture, initiating a grasp, controlling release, and calibrating the movement of their affected limb — their brain has no choice but to pay attention.
This is true motor learning.
The movement has to be intentional. It has to be effortful. It has to require the brain to figure out how to produce something it has lost the map for.
👉 That's not exercise.
👉 That's neuroplasticity in action.
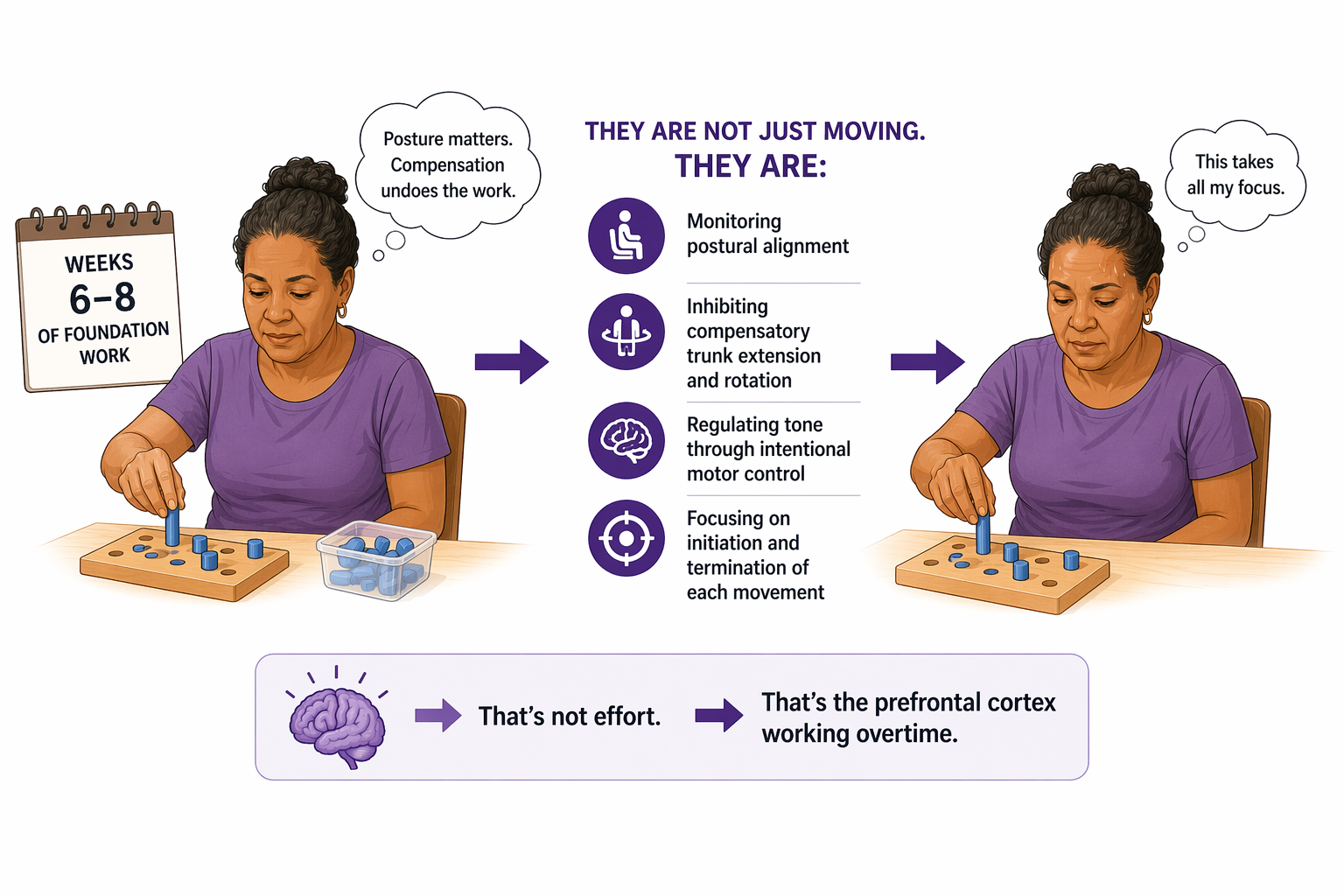
Why this is an attention intervention
Before this activity is appropriate, the patient has already spent weeks — often six to eight — on proximal tone inhibition. They already know posture matters. They already know compensation will undo the work.
👉 So when they sit down to do this task, they are not just moving.
They are:
— Monitoring postural alignment — Inhibiting compensatory trunk extension and rotation — Regulating tone through intentional motor control — Focusing on initiation and termination of each movement
That is sustained, selective, and divided attention — running simultaneously.
Your patient may sweat. Their hands may get clammy.
👉 That's not effort.
👉 That's the prefrontal cortex working overtime.
Why this is a dual tasking intervention
The unaffected hand stabilizes the power web.
👉 That is not a passive role.
By actively engaging the unaffected side in stabilization, you are inhibiting associated reactions — the tendency of the unaffected limb to mirror or compensate for what the affected side is doing. You are asking the brain to run two motor programs simultaneously: stabilize with one hand, produce refined isolated movement with the other.
Add the color-sequencing cognitive layer — and now you have a true motor-cognitive dual task.
👉 Motor demand: tone inhibition, grasp, reach, release 👉 Cognitive demand: working memory, sequencing, selective attention
This is the same dual tasking framework we covered last issue — just embedded in a meaningful upper extremity activity instead of a formal assessment.

How to Treat This (Real Sessions)
🔍 Establish the baseline first. Don't go straight to the activity. Confirm the patient already has isolated osteokinematic movements — shoulder flexion, internal/external rotation, elbow extension with pronation — before adding the functional layer.
🪑 Correct posture before every rep. Not once at the start. Before every single movement. Trunk compensation will undo the motor learning you're trying to build.
1️⃣ Start without the cognitive layer. Run the grasp-reach-place-release sequence without color sequencing first. Add the cognitive demand only after the motor pattern is consistent.
🛑 Block if you need to. If the patient keeps coming into abduction, use a belt with their permission. Modified constraint isn't failure — it's calibration.
🗣️ Name what you're seeing. If the fingers are swan-necking, tell the patient what's happening and why. They can handle it. Silence around tone presentation makes patients more anxious, not less.
💪 Let them sweat. Clammy hands and visible effort are signs the brain is working. Resist the urge to simplify too quickly.
Across Disciplines (Same System, Different Look)
This is OT-led — but the principles apply everywhere.
PT: any activity that asks a patient to perform a refined motor task while regulating posture, inhibiting compensatory movement, and following a sequence is running the same cognitive load. Dual tasking cost doesn't only show up during gait.
SLP: intentional motor control, initiation, and termination of movement are the same cognitive functions underlying oral motor control and word retrieval. The brain regions that regulate effortful movement overlap significantly with those that regulate effortful language production.
👉 One activity. One cognitive system. Different functional presentations.
Documentation
✏️ Name the defecits:
Patient demonstrated decreased information processing speed, requiring extended response time and repetition of verbal instructions throughout the session.
Link the function:
Deficits impacted ability to respond to safety cues during mobility tasks and complete multi-step daily activities in a timely and accurate manner.
Skilled intervention:
Clinician modified task presentation, pacing, and environmental demands to optimize processing and support safe functional performance.
Medical necessity:
Skilled intervention required to address cognitive processing deficits impacting safe and independent community and home functioning.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition

Member Resource: Power Web & Movement Integration Clinical Pack
What's included:
- Free resource: Stroke Upper Body — Understanding Spasticity (patient education, pages 1–3)
- Handout 1: Synergies of Hand Grasp — the full grasp pattern reference guide
- Handout 2: Stroke Upper Body Patient Resource (all 6 pages) — spasticity education, tone reduction techniques, upper limb recovery strategies, readiness milestones, and associated reactions
- Clinical application guide below — how to use each resource to set up, grade, and document the power web activity
Free Resource — Understanding Spasticity
(Pages 1–3)
Use this with your patient and their family before you ever introduce the power web.
Page 1 explains why spasticity is a brain signal problem, not a muscle problem — and why stretching alone doesn't fix it. This is the conversation that gets patient buy-in for why you're doing what you're doing.
Page 2 connects muscle stiffness, jerky movements, and fatigue to executive function and the reticulospinal tract — and explains why bright lights and noise make tone worse. Hand this to the family member who keeps wondering why their loved one "falls apart" in busy environments.
Page 3 is your tone reduction technique table — prolonged stretching, deep pressure, weight bearing, trunk rotation, slow movements, deep breathing, E-stim, and visual biofeedback. Use it as a session warm-up reference before moving into the activity.
👉 This is what happens before the power web comes out.
👉 Your patient needs to understand this first.
Handout 1 — Synergies of Hand Grasp
This is your activity grading reference. Before you set up the power web, identify which grasp pattern your patient is working toward. The activity in this newsletter is specifically designed for three-point/tripod grasp, prismatic pinch, and tip pinch — but the same setup can be adapted for lateral grasp, power disk grasp, or any other pattern depending on where your patient is in recovery.
Best used for: Identifying the target grasp pattern before the session, documenting the specific synergy being trained, explaining to patients and families exactly what functional movement you are rebuilding and why it matters for their daily life.
Clinical tip: Show the patient their target grasp on the chart before the session starts. Point to the everyday object that grasp pattern is used for — a pen, a cup, a pill bottle. Now the activity has a functional destination. That's not just motivating — it's encoding. The brain learns faster when the movement has meaning attached to it.
Handout 2: Stroke Upper Body Patient Resource (all 6 pages)
This is your full clinical decision-making resource for the power web activity. Here is how each page functions in context:
Pages 1–3 (spasticity education, tone reduction techniques): Use these as your session warm-up protocol. Before the power web comes out, your patient should have already completed at least one tone reduction strategy from page 3 — prolonged stretching, weight bearing, deep breathing, or trunk rotation. Do not skip this. Attempting the activity without tone reduction first means you are working against the nervous system, not with it.
Page 4 — Upper Limb Recovery Strategies: This is your clinical rationale page. The power web activity hits multiple strategies listed here simultaneously — bilateral task practice (stabilizing with the unaffected hand), cognitive-based retraining (the color sequencing layer), constraint-modified approach (blocking abduction with a belt when needed), and meaningful task engagement (connecting the grasp pattern to a real occupation using the synergy chart). Use this page to frame your clinical reasoning in documentation.
Page 5 — Key Milestones in Upper Limb Spasticity Recovery: This is your readiness checklist. Your patient must be at Milestone 4 — able to use their unaffected hand without producing tightness in the affected side — before the power web activity is appropriate. If they are not there yet, they are working on Milestones 1–3 first. Do not introduce the activity prematurely. Use this page to show the patient where they are in the progression and where the activity fits.
Page 6 — Associated Reactions: The newsletter explains that stabilizing the unaffected hand on the power web inhibits associated reactions in that limb. This page gives you the Brunnstrom framework to document where your patient is in recovery and why associated reaction management is a skilled clinical target — not a side effect — of this activity.
Best used for: Determining patient readiness, structuring the session sequence, connecting the activity to the broader recovery framework, and building the documentation narrative across all six pages.
Clinical tip: Milestone 4 on page 5 is your entry point for this activity — not a nice-to-have. If your patient cannot use the unaffected hand without pulling or producing tightness in the affected side, the stabilization role of the unaffected hand in this activity will backfire. Check Milestone 4 explicitly before starting.
Understanding and Treating Spasticity
Clinical Application Guide: Matching the Breakdown to Your Treatment
Before the session — tone reduction first
Pull page 3. Have the patient choose one or two strategies from the tone reduction table and complete them before picking up a single manipulative. Deep breathing plus prolonged stretching is a reliable starting combination. Time it. Document it. This is skilled intervention, not a warm-up.
Setting up the activity — identify the grasp first
Pull Handout 1. Point to the target grasp pattern. Name it with the correct terminology. Tell the patient which everyday object uses that grasp. Set up the power web with the pipe connectors and spread the targets on the patient's affected side or across the surface depending on whether you are also targeting visual scanning.
During the activity — use the milestone framework
Keep page 5 visible. You are working at Milestone 4. If the patient's tone increases significantly in the affected hand while the unaffected hand stabilizes, slow down — you have exceeded their current recovery stage. Reduce the resistance level, simplify the target layout, or remove the cognitive color-sequencing layer until stability is reestablished.
Adding the cognitive layer
Only after the motor pattern is consistent without color sequencing. Add color sequence instructions verbally: red first, blue second, green third. This introduces the working memory and selective attention demands that make this a dual-task cognitive intervention. Do not add this layer on the first session.
Documenting associated reactions
Use page 6 and the Brunnstrom framework. If you see associated reactions in the unaffected limb decreasing as the session progresses, that is a documented skilled outcome — not incidental. Name it: "Decreased frequency of associated reactions in the unaffected upper extremity with stabilization demand during fine motor task, consistent with progression from Brunnstrom Stage 3 toward Stage 4."
Documentation Language
✏️ Name the deficit: Patient demonstrated flexor synergy patterning in the affected upper extremity with associated reactions in the unaffected limb during fine motor task demands, limiting isolated joint control and functional grasp.
🔗 Link to function: Deficits impacted ability to perform tasks requiring three-point grasp, pinch, and bilateral upper extremity coordination in daily activities including dressing, grooming, and meal preparation.
🔥 Skilled intervention: Clinician implemented tone reduction protocol followed by graded resistive fine motor activity targeting tripod/prismatic pinch grasp reintegration, with cognitive dual-task layer added to address motor learning and attentional demands of movement reintegration.
⚕️ Medical necessity: Skilled intervention required to address flexor synergy, associated reaction inhibition, and grasp reintegration — task grading, cognitive load, and real-time clinical judgment cannot be replicated through unskilled instruction or home exercise alone.
One-Line Clinical Reasoning Starters
Use these when documenting medical necessity or justifying continued skilled care:
-
Grasp reintegration at the level of tripod and pinch patterns requires skilled neuromuscular facilitation and real-time task grading beyond the scope of unskilled practice.
-
Tone reduction prior to fine motor activity is a clinical prerequisite — sequencing and monitoring this process requires skilled judgment to avoid reinforcing abnormal movement patterns.
-
Associated reaction inhibition during bilateral task practice is a skilled outcome requiring ongoing clinical monitoring of Brunnstrom staging and motor response.
-
Cognitive-based retraining embedded in upper extremity activity addresses the brain-movement connection — this cannot be achieved through repetitive exercise alone.


Responses