
You give an instruction.
You wait.
And wait.
Then — finally — they respond.
Or they stop walking when you talk to them.
Or they need everything repeated twice.
Or they do fine in a quiet room but fall apart in the hallway.
👉 This is not confusion.
👉 This is not hearing loss.
👉 This is not noncompliance.
This is information processing speed — and it's one of the most overlooked cognitive factors in everyday rehab.
🐢 Slowed processing speed is one reason the attention system gets overwhelmed — and when attention breaks down, nothing gets stored in the first place. Next issue, we're going deeper into where that pipeline actually fails.
So what is information processing speed?
Think of it as your brain's bandwidth.
How fast can it take in information, make sense of it, and produce a response?
It's not about intelligence.
It's not about effort.
It's about the speed of the underlying hardware — specifically, the white matter pathways that connect brain regions to each other.
When those pathways are intact, signals travel fast.
👉 When they're disrupted — by aging, TBI, stroke, MS, or dementia — everything slows down.
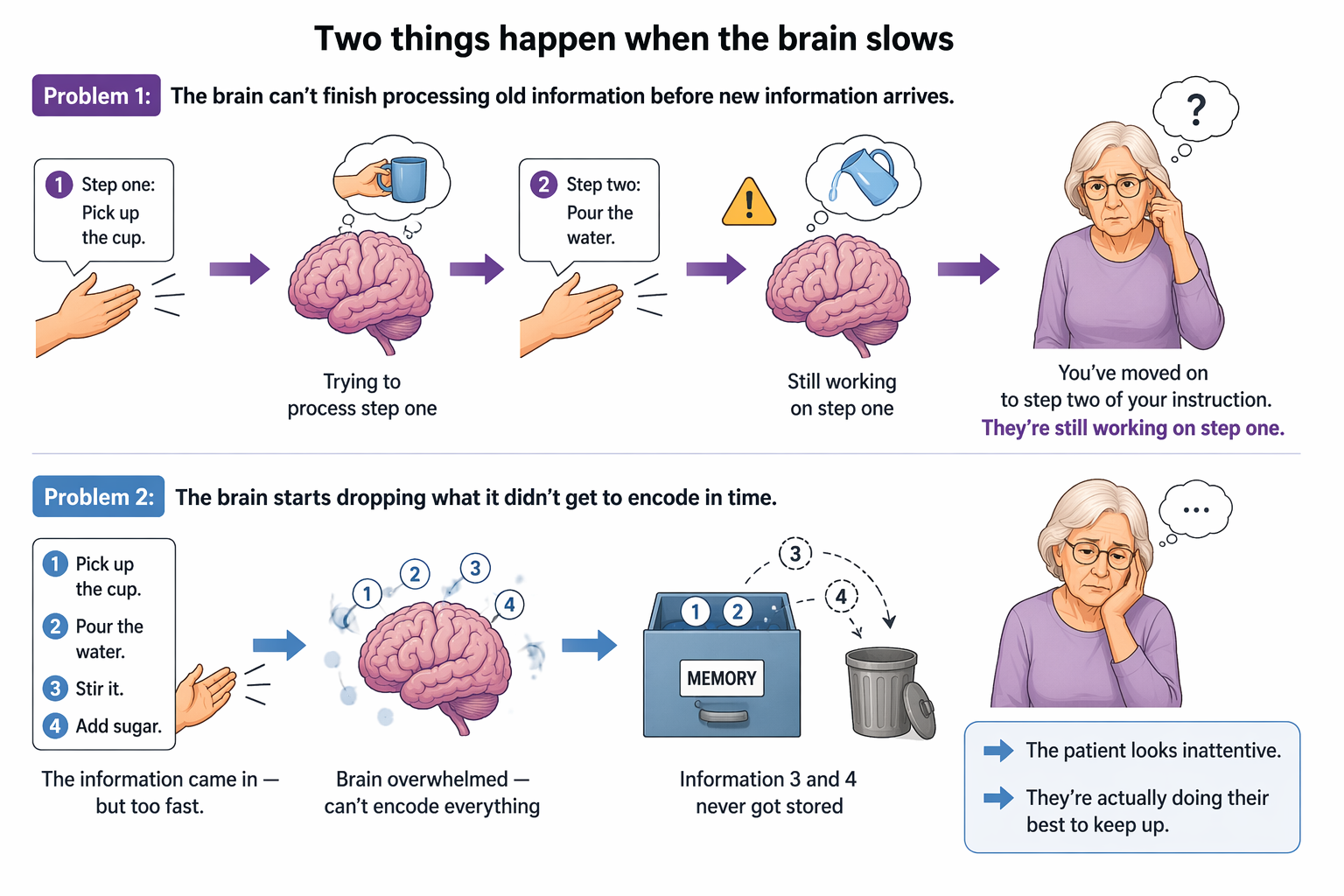
Two things happen when the brain slows
Problem 1: The brain can't finish processing old information before new information arrives.
You've moved on to step two of your instruction.
They're still working on step one.
Problem 2: The brain starts dropping what it didn't get to encode in time.
The information came in — but too fast.
It never got stored.
👉 The patient looks inattentive.
👉 They're actually doing their best to keep up.
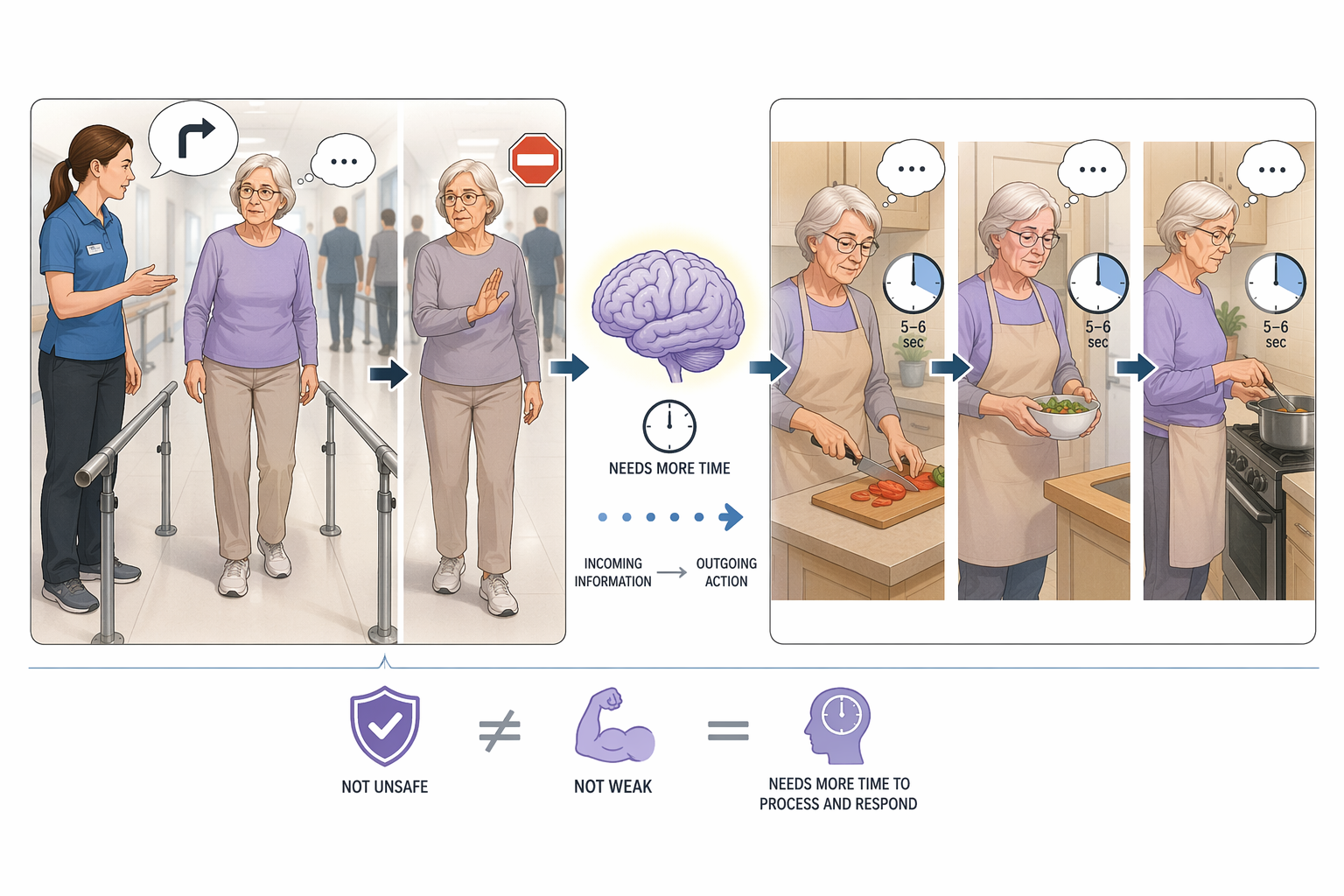
Clinical snapshot:
Margaret is a 72-year-old in outpatient PT after a fall. She's alert, pleasant, scores 27/30 on her MoCA. But her PT notices she takes 5–6 seconds to respond to verbal cues during gait training — and when those cues come quickly in a busy hallway, she stops walking entirely. Her OT sees the same thing during meal prep: she can complete each step, but needs extra time between them before she can move on. Margaret isn't unsafe because she's weak. Her brain needs more time between incoming information and outgoing action.

How to Treat This (Real Sessions)
🐢 Slow down your own pace. One cue at a time. Wait for a full response before adding more. Silence is not awkward — it's processing time.
🔇 Reduce environmental noise. IPS deficits are magnified in busy, loud, or visually distracting environments. A quiet room shows the true baseline.
🧠 Grade by cognitive demand, not just physical difficulty. A patient may be able to walk AND talk — just not at full speed. Build up to dual tasks intentionally.
📝 Use written or visual supports. When verbal processing is slowed, written cue cards or visual sequences reduce the real-time load.
💗 Don't mistake slowness for inability. They may get there — they just need more time than the environment is giving them.
Across Disciplines (Same System, Different Look)
PT: patient freezes mid-gait when you give a verbal cue. Dual-task walking slows significantly or becomes unsafe.
OT: patient manages tasks in a quiet room but falls apart in a stimulating environment. Instructions don't carry from one step to the next.
SLP: patient needs everything repeated — not due to hearing or comprehension, but because they need more time to process what was said before they can respond.
Documentation
✏️ Name the defecits:
Patient demonstrated decreased information processing speed, requiring extended response time and repetition of verbal instructions throughout the session.
Link the function:
Deficits impacted ability to respond to safety cues during mobility tasks and complete multi-step daily activities in a timely and accurate manner.
Skilled intervention:
Clinician modified task presentation, pacing, and environmental demands to optimize processing and support safe functional performance.
Medical necessity:
Skilled intervention required to address cognitive processing deficits impacting safe and independent community and home functioning.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition

Member Resource: Processing Speed Clinical Pack
What's included
Handout 1: Attention & Memory — a 4-page patient-ready resource covering how memories form, types of memory, and the attention hierarchy
PhD Candidate, Rehabilitation Science
Handout 2: Dual Tasking Assessments and Interventions — a full clinical tool with two structured assessments, dual tasking cost calculation, and a motor + cognitive task menu
Clinical application guide below — matching the specific IPS breakdown to your treatment approach
Reminder: You do NOT treat "slow processing."
You treat what the slowness is doing to function.
👉 Is it breaking down dual-task safety?
👉 Is it preventing new information from being encoded?
👉 Is it causing the patient to miss instructions entirely?
Each of those has a different treatment target.
Here's how to use your resources to address each one.
Handout 1 — Attention & Memory Resource (4 pages)
Use this with patients and families to explain why working on attention and processing speed comes before memory work. Walk through the "how do you make a memory?" sequence: attention → encoding → storage → consolidation → retrieval. Use the attention hierarchy page to show the patient exactly where the breakdown is happening.
Best used for: Patient and family education on why instructions aren't sticking; identifying which level of attention is failing; setting cognitive goals the patient can see and track.
Clinical Tip: The types of memory page is especially useful for distinguishing procedural from episodic from prospective memory failures — and for explaining to families why "they can do their exercises but can't remember our conversation." Circle the relevant memory type and use it as a goal anchor across disciplines.
How to Make a Memory Education PDF
Handout 2: Motor-Cognitive Dual Tasking Practitioner Guide
This resource has three parts: two structured assessments that establish a baseline and calculate dual tasking cost, a motor task menu, and a cognitive task menu — with pre-built combinations across all task types.
Assessment 1 pairs tandem gait (timed over 20–40ft) with digit span retention (baseline 4 digits, goal 8–10). Assessment 2 pairs a 10-movement arm sequence crossing midline with unrelated word recall (baseline 3 words, goal 8). Both calculate dual tasking cost by comparing motor-only time to dual-task time.
Dual Tasking Cost = Motor Only Time - Dual Task Time
Best used for: Establishing a quantifiable baseline for dual-task performance; grading cognitive load across sessions; building toward real-world demands using the motor + cognitive combination menu.
Clinical Tip: The dual tasking cost number is your functional safety metric — not just a cognitive score. A patient with a significant cost (motor slows substantially under cognitive load) is telling you their processing speed is insufficient to handle both channels simultaneously. Document it as a functional safety finding, not just a cognitive one, and use it to justify continued skilled intervention.
Motor Cognitive Dual Tasking Resource
Clinical Application Guide: Matching the Breakdown to Your Treatment
IPS affecting instruction-following and encoding
What you'll see: patient misses steps, needs immediate repetition, or responds to something other than what was asked.
Use Handout 1 (attention hierarchy, page 1) to identify the attention level failing. Then use the cognitive task menu in Handout 2 — start with memory tasks (digit recall, word lists) as single-channel practice before pairing with any motor demand. Do not add a motor layer until the cognitive baseline is established.
IPS affecting motor-cognitive dual-task safety
What you'll see: patient is safe during isolated movement but slows, stops, or makes errors when a cognitive demand is added simultaneously.
Run Assessment 1 (tandem walk + digit span) or Assessment 2 (arm sequence + word recall) to get a baseline and calculate dual tasking cost. Use the pre-built motor + cognitive combinations from the intervention menu to systematically grade up — starting with walking + counting, then advancing to balance + attention tasks or agility + language tasks as performance improves. Never skip to a harder combination without establishing cost at the current level.
IPS affecting carryover across sessions
What you'll see: patient performs well in session, returns next visit with no recall of what was practiced.
Use Handout 1 (page 1) to explain consolidation failure — information not processed fast enough never got stored. In Handout 2, focus the cognitive element on memory tasks (digit sequences, unrelated word lists) with an intentional delay built in — the assessment already structures this with a timed hold between encoding and recall. Increase session frequency before increasing task complexity.
IPS affecting performance in high-stimulation environments
What you'll see: patient is accurate and safe in a quiet clinic room, but performance drops in the hallway, gym, kitchen, or community.
Use the Handout 2 combination menu to grade in controlled interference before transitioning to real environments: balance + attention tasks and strength + decision-making introduce cognitive load during postural or physical demand in a way you can still control. Use dual tasking cost from Assessment 1 or 2 as the benchmark for when the patient is ready to advance to uncontrolled environments.
Documentation Language
✏️ Name the deficit: Patient demonstrated decreased information processing speed with delayed response to verbal instruction and measurable dual tasking cost on structured assessment.
🔗 Link to function: Deficits impacted ability to safely perform motor tasks under concurrent cognitive demands, consistent with real-world functional environments.
🔥 Skilled intervention: Clinician administered standardized dual task assessment to establish baseline, calculated dual tasking cost, and implemented graded motor-cognitive protocol with systematic progression of task complexity.
⚕️ Medical necessity: Skilled intervention required to quantify and address dual-task deficits secondary to reduced processing speed, impacting safe and independent functioning in home and community environments.
One-Line Clinical Reasoning Starters
Use these when documenting medical necessity or justifying continued skilled care:
-
Calculated dual tasking cost indicates motor performance is significantly impaired under concurrent cognitive load, placing the patient at risk during unsupervised real-world activities.
-
Decreased processing speed creates a narrow encoding window, limiting the patient's ability to consolidate new safety strategies across sessions without structured repetition.
-
Graded motor-cognitive protocol requires skilled judgment to advance task combinations appropriately based on dual tasking cost — not appropriate for unskilled instruction.
-
Processing speed deficits under divided attention conditions cannot be adequately addressed through compensatory strategies alone at this stage of recovery.


Responses