
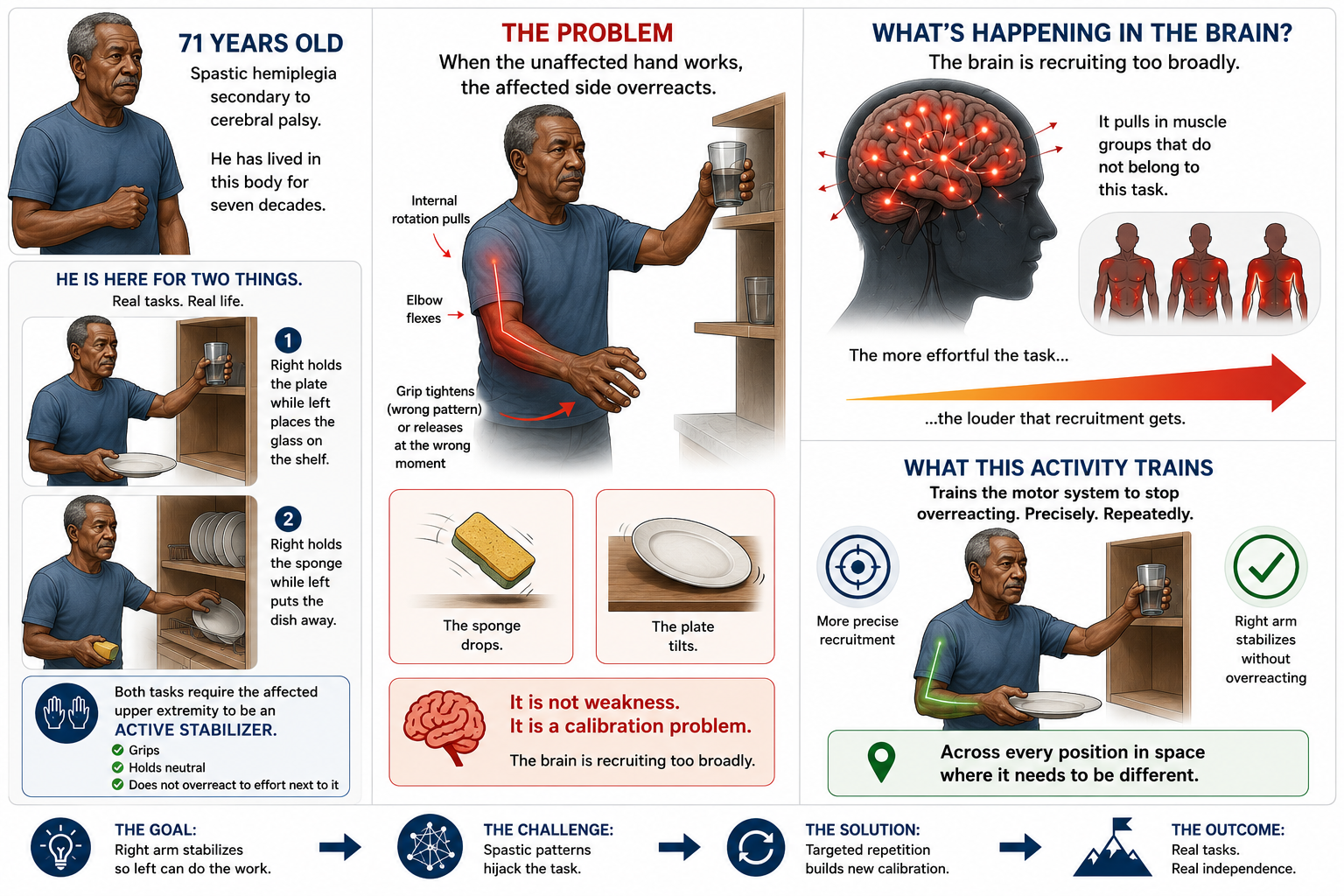
Your patient is 71 years old. He has spastic hemiplegia secondary to cerebral palsy. He has lived in this body for seven decades.
He is not here because he wants to recover from something that just happened. He is here because there are two things he cannot do — and they are not abstract goals on a chart. He wants to hold a plate with his right hand while his left places a glass on the shelf. He wants to hold a sponge with his right hand while his left puts the dish away.
Both of those tasks require the same thing: the affected upper extremity has to function as a stabilizer while the other hand does the work.
Not a passive stabilizer. An active one — one that grips, holds neutral, and does not respond to the effort next to it by driving further into the spastic pattern.
That is the problem. When the unaffected hand loads up — when it grips, lifts, or moves through space — the affected side reads that effort and responds with increased tone. Internal rotation pulls. The elbow flexes. The grip tightens in the wrong pattern or releases at the wrong moment. The sponge drops. The plate tilts.
It is not weakness. It is a calibration problem.
👉 The brain is recruiting too broadly. It is pulling in muscle groups that do not belong to this task. And the more effortful the task, the louder that recruitment gets.
This activity trains the motor system to stop doing that. Precisely. Repeatedly. Across every position in space where it needs to be different.
*BOT Portal Members can download this image on the BOT Portal Google Drive [Click Image]
What the activity actually is
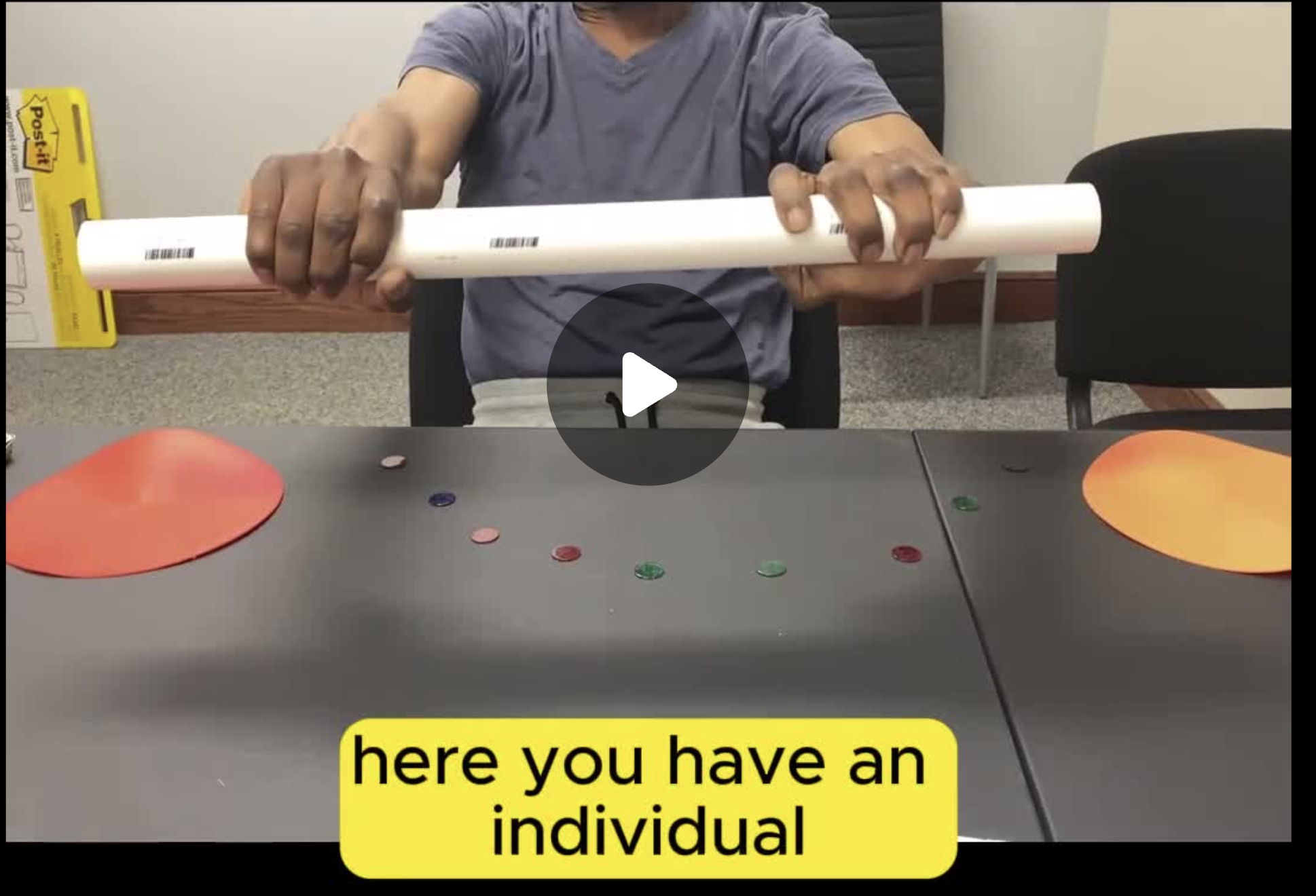
The tools:
🔵 Bingo chips — arranged in a rainbow arc across the tabletop, one chip per position, spaced to create a clear left-to-right spatial progression
🔩 One 20-inch PVC pipe — the cylindrical grasp scaffold for the primary intervention phase
🟠 Two poly dots — placed at either side of the arc as bilateral anchors for the opening movement phase
⏱️ A timer
📋 A tracking sheet: which positions were completed, where tone increased, where grasp quality changed, time to complete the arc, number of position errors
The setup:
Bingo chips are placed in a fixed arc on the tabletop before the patient sits down. The arc is not random. It is a deliberate spatial sequence — the chips begin at the patient's midline and extend outward in both directions, or begin ipsilaterally and arc across to contralateral space, depending on which spatial range you are targeting this session. The position of every chip is documented and replicated at every session.
Poly dots are placed at the bilateral endpoints. These are where the session begins.
The task, in two phases:
Phase one — bilateral synchronous AROM.
The patient begins at both poly dots simultaneously. Both hands move together, symmetrically, through the full arc and back. This is not warm-up. This is tonal priming — large, bilateral, synchronous movement activates reciprocal inhibition across both sides and provides the sensorimotor baseline before the more demanding unilateral phase begins. This phase runs until the quality of movement is consistent and the affected side is not driving into the spastic pattern at rest.
Phase two — unilateral arc sequencing with the pipe.
The patient takes the 20-inch PVC pipe in the affected hand. One hand only. The task is to hover the pipe directly over each bingo chip, in sequence, moving across the arc. The pipe must cover the chip before the patient moves to the next position. No rushing. No skipping. Every chip is a full stop.
👉 That is the entire task — and what it demands from the nervous system is not simple at all.
Before the first chip is covered — lead with science every time
He has been living with this body for over seventy years. He knows what it does. He knows the pull. He has been managing it, compensating for it, and working around it for decades.
He does not need to be told he has spasticity. He needs to understand what you are doing about it, and why this particular activity is the right tool for this particular problem.
Before the pipe is picked up, say this:
"When you try to use the plate at home — when your left hand is working and your right is supposed to hold still — what happens is that your brain sends a signal to your right arm that it doesn't need to send. Your muscles over-recruit. They pull in more than the task asks for. What we're doing right now is teaching your brain to recalibrate that signal, to recruit exactly the right amount for each position. Every time you move the pipe to a new chip, your brain has to re-solve the problem for that exact position in space. The more times you solve it, the better your brain gets at sending the right signal instead of the loud one."
👉 That is not motivation. That is encoding. The patient who understands that every chip position is a new calibration problem is practicing differently than the patient who thinks he is hovering a pipe over dots.
The science matters especially here, because this patient has been told — by years of lived experience — that the arm does what it does. Part of the clinical intervention is changing that expectation at the neurological level. Neuroplasticity in the context of longstanding spasticity is real, it is slower, and it requires the patient to be a participant in it, not a recipient of it.
Name what you are doing. Every session.
Why the arc structure is the intervention
The bingo chips are not targets. They are calibration checkpoints.
Here is what happens when the patient moves the pipe from one chip to the next:
The position in space changes. The shoulder angle changes. The elbow angle changes. The distance from midline changes. The demand on the rotator cuff, the anterior deltoid, and the forearm musculature changes. And the amount of tonal pull the spastic pattern exerts on that position changes — because spasticity is not uniform across the full range of motion. It has peaks. It has positions where the pull is strongest, where the compensations appear, where the cylindrical grasp quality degrades.
👉 The arc reveals the map of those peaks. Chip by chip.
Most patients find a consistent position on the arc where things change. It might be when the pipe crosses midline. It might be in the outermost contralateral chips where the shoulder is most challenged. It might be in the midrange chips, where the elbow flexion pattern is most available to the spastic pull. Whatever it is, it is consistent, and it is specific to that patient's muscle group involvement.
That position is your treatment target. Not the arc in general, but that specific chip, that specific position in space, that specific demand on the shoulder and forearm at that angle.
Document which chip it is. Return to it. Spend more time there. Approach it from both directions — from the ipsilateral side and from the contralateral side — and note whether the approach direction changes the quality of the transition into that position. It usually does. That difference is data.
Why this is a tonal inhibition intervention

*BOT Portal Members can download this image on the BOT Portal Google Drive [Click Image]
Sustained cylindrical grasp while maintaining neutral shoulder rotation is not the default for a patient with spastic hemiplegia. The default is internal rotation at the shoulder, elbow flexion, forearm pronation, and — depending on the patient — wrist flexion with finger curling.
The pipe scaffolds the grasp. Its diameter and weight are selected to match the patient's current cylindrical grasp capacity — large enough that the finger extensors are not overwhelmed, heavy enough that the forearm is loaded, light enough that fatigue doesn't collapse the pattern before you can work in it.
Keep Your Eye On The Targets
Watch the shoulder from the moment the hand closes around the pipe.
The shoulder is where the session actually lives. The hand will look like it is working — it is holding, it is moving, it is doing something visible. The shoulder is where the inhibition is being tested. If the shoulder begins to internally rotate the moment the pipe loads (i.e., before the first chip is reached) you have your finding. The inhibitory control threshold is below the load of the pipe itself. That is your baseline.
If the shoulder holds neutral through the first three chips and then drifts on the fourth...that is a different finding. The inhibitory control threshold is at approximately chip four under this load. That is your endurance threshold for tonal inhibition, and it is the number you are moving across this plan of care.
Watch the elbow simultaneously. The flexion pull is the partner to the internal rotation pull — they travel together in the spastic pattern. When the shoulder starts to give, the elbow is usually close behind. Note whether shoulder drift precedes elbow drift, or whether they move together. That sequence tells you which muscle group is anchoring the pattern and which is following it.
The forearm is where the refinement lives. Pronation and supination (forearm rotation) is the movement the patient is working on distally while the shoulder holds neutral proximally. The pipe is long enough that both demands are simultaneously active: the proximal system is maintaining neutral while the distal system is working. Neither can rest while the other operates.
👉 That is the functional equivalent of holding a plate while the other hand moves. The proximal system sustains. The distal system acts. The affected side has to do both (hold the proximal pattern and allow the distal movement) without the tonal system collapsing the two into one loud, undifferentiated recruitment.
Why every chip position is an executive function demand
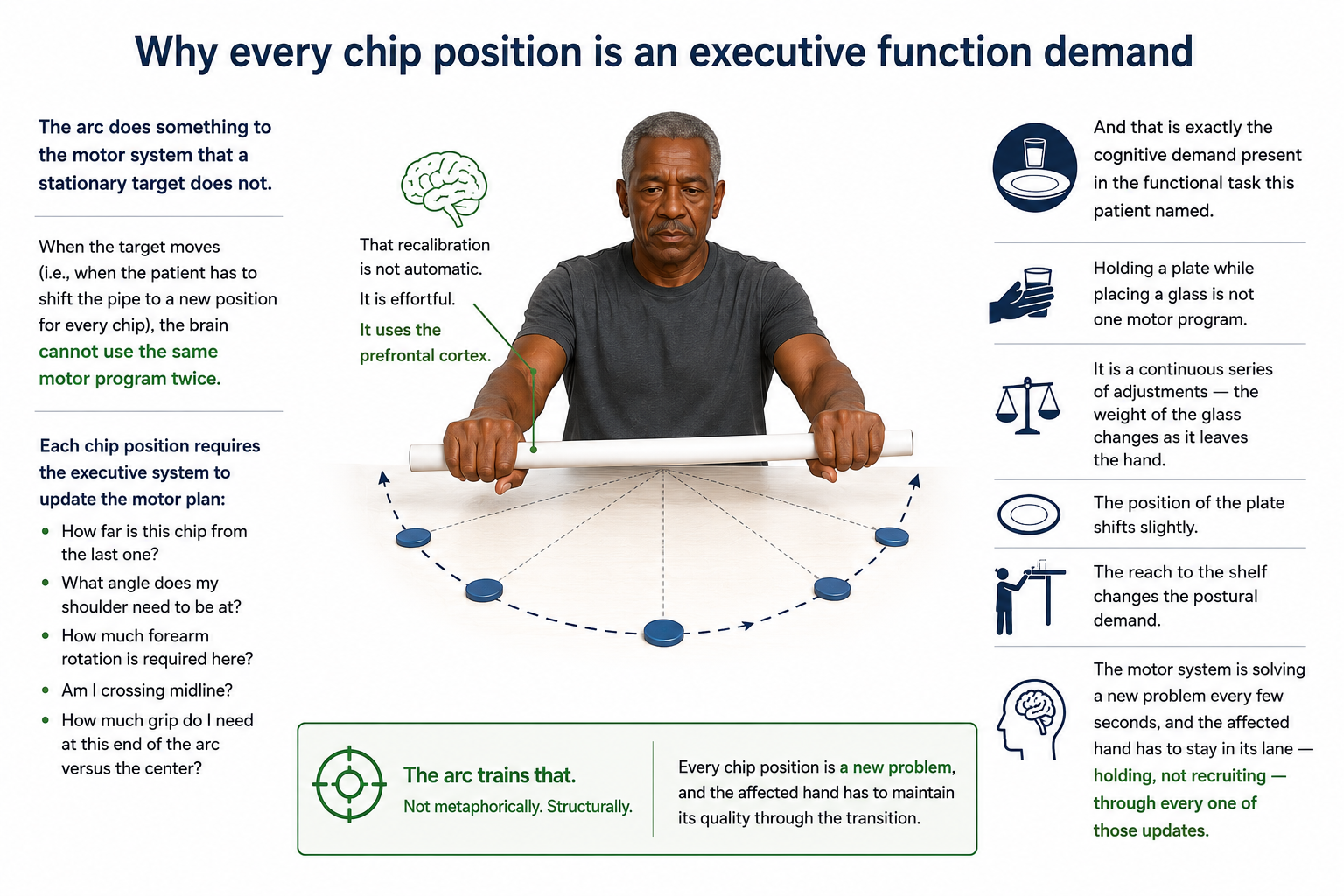
The arc does something to the motor system that a stationary target does not.
When the target moves (i.e., when the patient has to shift the pipe to a new position for every chip), the brain cannot use the same motor program twice.
Each chip position requires the executive system to update the motor plan: how far is this chip from the last one, what angle does my shoulder need to be at, how much forearm rotation is required here, am I crossing midline, how much grip do I need at this end of the arc versus the center.
👉 That recalibration is not automatic. It is effortful. It uses the prefrontal cortex.
And that is exactly the cognitive demand present in the functional task this patient named. Holding a plate while placing a glass is not one motor program. It is a continuous series of adjustments (e.g., the weight of the glass changes as it leaves the hand, the position of the plate shifts slightly, the reach to the shelf changes the postural demand). The motor system is solving a new problem every few seconds, and the affected hand has to stay in its lane — holding, not recruiting — through every one of those updates.
The arc trains that. Not metaphorically. Structurally. Every chip position is a new problem, and the affected hand has to maintain its quality through the transition.
👉 Document where the motor plan breaks down, not just where the tone increases. A patient whose grip quality is excellent at the first three chips and then collapses at chip four (not because of tone, but because of a motor planning failure in the transition) has a different intervention target than a patient whose tone pulls him off course at the same chip. Both break at chip four. They break for different reasons.
Why the bilateral-to-unilateral progression is not a warm-up

Phase one — bilateral synchronous AROM — is not preparation for the real activity. It is the first clinical intervention of the session.
Bilateral synchronous movement activates the interhemispheric pathways that support reciprocal inhibition. When both limbs move together in the same pattern, the nervous system is being asked to organize symmetrical output — which temporarily reduces the asymmetric tonal dominance that drives the spastic pull on one side. The affected side, moving in synchrony with the unaffected side, receives organizing input from the contralateral system.
This is not always visible in the movement. The patient may not look dramatically different during phase one.
But the tonal baseline at the start of phase two — the moment the pipe is moves to a one-hand hold — is different when phase one has been completed cleanly than when phase one has been rushed or skipped.
👉 Do not skip phase one when you are running behind. Shorten the number of chips in phase two. Phase one is not the preamble — it is the neurological setup that makes phase two achievable.
Track whether phase one quality predicts phase two tonal threshold. Over time, across sessions, a patient whose bilateral phase is clean should be showing an expanding tonal inhibition window in phase two.
If that relationship is not appearing, the bilateral quality is not as clean as it looks. Go back and look harder at what the affected side is doing during phase one — whether it is matching the unaffected side or whether it is riding along at a lower amplitude or a slightly different rotation angle.

How to Treat This (Real Sessions)
🔵 Run the bilateral phase until quality is consistent — not until a fixed number of repetitions is complete. The endpoint of phase one is not the clock. It is the affected side moving in genuine synchrony: matching speed, matching rotation, not lagging, not compensating. If that takes two passes across the arc, stop at two. If it takes eight, run eight. The number that gets you clean entry into phase two is the right number, and it belongs in your note.
👉 Watch the affected shoulder during phase one, not the hands. The hands will look like they are keeping up. The shoulder will tell you whether the nervous system is organizing symmetrically or whether the affected side is performing approximate synchrony while the tonal system is already loading up. A shoulder that is two degrees of internal rotation shy of matching the unaffected side during phase one is a shoulder that will hit its tonal ceiling three chips earlier in phase two. That difference is predictable and documentable.
📐 Set the arc before the patient sits down and do not change it mid-session. The chip positions are your spatial variables for this session. The patient's brain is building a spatial map of the arc from the moment he sees the table. That map is part of the executive function scaffold for the task. Changing chip positions mid-session does not increase the difficulty, it resets the motor planning context and makes your within-session comparison meaningless. Spatial progressions belong between sessions, with full documentation of the new arc configuration.
🧠 Identify the breakdown chip before the session ends and return to it deliberately. If chip five is where the shoulder internally rotates, do not just note it and move on. Approach chip five from chip four again. Then again. Then approach it from chip six. Work the transition into and out of that position until the tonal response at that chip reduces, holds reduced, or you have sufficient data to know it is not budging this session. That repetition at the hard position is the intervention, not the completion of the full arc.
🔄 Grade the pipe load and the arc width on completely separate tracks. If you are extending the arc further into contralateral space this session, the pipe stays the same weight. If you are adding a heavier pipe, the arc width stays the same as last session. One variable. One session. Advancing both simultaneously means you cannot attribute the change in performance to either variable. Treat the progression the way you would treat exercise prescription...one parameter at a time, with documented rationale.
🖐️ When you see the internal rotation pull — name it in the moment, without alarming the patient. "There it is — do you feel that pull at the shoulder? That's the signal we're working on. Can you bring it back to neutral? Hold it there." Then document whether the patient could self-correct to neutral with verbal cuing, and whether the correction held through the next chip or collapsed again immediately. The cueing response is your motor learning data. A correction that holds for two chips and then drifts is different from a correction that collapses before the pipe reaches the next chip — document both, and track the difference session to session.
📊 Track four variables every session: breakdown chip, shoulder drift pattern (gradual or sudden), cueing response (self-correct or required external cue, correction duration), and forearm rotation quality at the breakdown position. They move independently and they tell different stories. A patient whose breakdown chip advances from chip four to chip six but whose cueing response degrades has made an endurance gain while losing self-monitoring. Those are two different findings. Both belong in the note.
Across Disciplines (Same System, Different Look)
This is OT-led — but the motor modulation and executive function architecture apply across disciplines.
PT: If this activity is performed with the patient standing at the table — or seated on an unstable surface, or standing with weight shifted toward the affected side — the postural demand compounds the tonal inhibition demand. The inhibitory control threshold will be earlier. The breakdown chip will move. Document the postural condition as a controlled variable for every session — supported sitting, unsupported sitting, standing, standing with affected-side weight shift — and track how postural load changes the tonal inhibition window. That interaction is your dual-task postural-motor data, and it is directly relevant to discharge planning if the patient's functional goals occur in standing.
SLP: The executive function architecture of this task — holding a spatial map across a sequenced motor task, recalibrating the motor plan at each position, self-monitoring whether the affected side is staying in pattern — is the same cognitive architecture required for sequenced ADL performance under motor load. A patient who loses the chip sequence while managing the tonal demands is showing executive function failure under concurrent motor load. If your patient has aphasia or executive function deficits alongside the motor presentation, his ability to hold the spatial sequence of the arc while managing bilateral and then unilateral motor demands is a direct cognitive-motor measure. The breakdown point on the arc is not just a motor finding...it is a cognitive-motor ceiling. Being able to perform a complete cognitive-motor task while also being able to hold a conversation is going to be very difficult and something worth addressing.
👉 One pipe. One arc of chips. Three disciplines worth of data.
When the pipe becomes a plate
The arc does not stay a drill. That is the point.
The progression from the PVC pipe to functional objects is the bridge from the treatment table to the kitchen shelf...and it is not a reward at the end of the protocol. It is a planned, graded transition that belongs in the treatment plan from the first session.
The pipe is the entry point because it is standardized. Its diameter is fixed. Its weight is fixed. Its surface is uniform. It gives you a clean baseline.
Once the patient can complete the full arc with the pipe (i.e., sustaining neutral shoulder rotation through all positions, with minimal cueing, with forearm rotation quality intact at the breakdown chip) the pipe is no longer the right tool. It is too easy. The nervous system has learned this object in this arc. It needs a new calibration problem.
The first substitution is a plate at the lowest functional weight (a salad plate, empty, held at a consistent grip. The grip changes. The object changes. The arc stays exactly the same. One variable.
Then the plate at increasing weights. Then the plate at different levels (the arc extended vertically, not just horizontally, because the shelf is not at tabletop height). Then a cup with fluid in it (because fluid shifts, and the motor system has to recalibrate mid-movement to stay level). One chip, one cup, with a small amount of fluid. Then more fluid. Then a full cup at each chip position along the arc.
👉 That is not a grading strategy. That is a reconstruction of the task he named in intake — holding a plate while placing a glass, holding a sponge while putting the dish away — built back up, piece by piece, from the arc that trained the system to stop over-recruiting.
Document the object transition explicitly. When the pipe is retired, name what replaced it, at what weight, and what the tonal inhibition threshold was at the new object. The threshold will shift — it usually gets earlier when the object changes, even when the arc stays the same. That regression is not failure. It is data. It is the calibration problem presenting itself at the new level.
Documentation
🧠 Document the system — not just the task.
This is not a PVC pipe exercise.
Identify and document:
— tonal inhibition: sustained cylindrical grasp under concurrent forearm rotation demand, shoulder internal rotation threshold by chip number, cueing response and correction duration
— motor modulation: recalibration of recruitment across sequential arc positions, executive function demand of spatial sequencing under concurrent tonal management, breakdown position and approach-direction effects
— bilateral-to-unilateral progression: quality of synchrony during phase one, relationship between phase one quality and phase two tonal threshold, interhemispheric activation as clinical preparation for unilateral demand
👉 If you don't name it, it doesn't exist clinically.
📍 Describe where the breakdown occurs — specifically.
Don't write "patient had difficulty with the activity."
Write what actually happened:
— shoulder internal rotation observed at chip 5 of 9, gradual drift onset over 3-4 seconds, not self-detected prior to clinician cuing
— verbal cuing to neutral achieved correction; correction held through chip 6 before drift recurred
— forearm rotation quality (pronation range) decreased by approximately 30% at and beyond chip 5 position; tip of arc not reached this session
— bilateral phase required 6 passes before affected shoulder achieved consistent neutral matching
— phase two tonal threshold corresponded with phase one pass count as previously observed
👉 Each of these is a specific, measurable, functionally meaningful clinical finding.
📏 Measure the tonal inhibition threshold every session.
Document:
— chip number at which shoulder internal rotation was first observed
— whether drift was gradual or sudden
— whether patient self-detected the drift or required external cuing
— correction duration following cuing
— whether threshold changed based on approach direction (ipsilateral vs. contralateral approach to breakdown chip)
👉 An increase in breakdown chip number across sessions is a measurable tonal inhibition endurance gain with a direct functional correlate — it means the affected limb is holding pattern longer before the spastic recruitment overrides the voluntary inhibition. Track it every session. It is your primary motor outcome variable at this stage.
⚖️ Document the object transition when it occurs.
— object used this session (pipe, plate, cup, weighted variant)
— object weight and fill level if applicable
— tonal threshold at the new object compared to last object
— arc configuration used
👉 The threshold regression at object transition is not a setback. Document it as a recalibration demand, the nervous system is re-solving the problem at a new level. That is the intervention working as designed.
🔄 Capture the bilateral-phase data separately from the unilateral-phase data.
— number of bilateral passes required to reach consistent synchrony
— quality marker used to define clean synchrony (shoulder match, rotation match, speed match)
— whether phase one quality predicted phase two threshold this session
👉 Over time, the relationship between phase one quality and phase two threshold is your most sensitive early indicator of transfer. A patient who achieves clean synchrony in fewer bilateral passes and whose phase two threshold is expanding is showing neurological reorganization, not just strength or endurance gain. Document it as such.
🧾 Tie it to function. Every note. Every session.
Make the connection explicit:
— stabilization of the affected upper extremity during bilateral household task performance (holding plate, sponge, cup while contralateral hand operates)
— tonal management across a range of shoulder positions and object weights relevant to kitchen and ADL environments
— recalibration of motor recruitment across spatial positions replicating the variable demand of functional reach and stabilization tasks
👉 This is not a tabletop arc drill.
👉 This is tonal inhibition and motor modulation training with a direct, nameable line to the bilateral upper extremity functional performance this patient named on day one.
Close every note with that line. The moment the functional connection becomes implicit (the moment you assume the reader will make it themselves) is the moment your documentation stops justifying skilled care.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!
What's included:
Resource 1: Stroke Upper Body Patient Resource — your patient-facing education library covering what spasticity is, why stretching alone doesn't work, strategies to decrease tightness, upper limb recovery milestones, and associated reactions. Six pages, each designed to be pulled individually based on where the patient is in their recovery.
Resource 2: Arc Progression Reference — your session-side clinician tool mapping all six object levels of the arc activity, with the new variable being introduced at each level, observation targets, advance criteria, and fill-in documentation language for every stage.
Clinical application guide below — how to use both resources together to set up, grade, document, and progress the arc activity across your plan of care.
Handout 1 — Stroke Upper Body Patient Resource
This is not a handout you give the patient on day one and never reference again. It is a library — six pages, each designed for a specific moment in the recovery arc. Pulling the right page at the right time is a clinical decision, not an administrative one.
Best used for: Staged education that matches where the patient is neurologically and behaviorally. The wrong page at the wrong stage creates confusion or, worse, a patient who thinks the prognosis is fixed. The right page at the right moment creates a patient who understands what is happening in their own body — and who can therefore participate in retraining it.
Which page, and when:
"What Causes Spasticity" — this is your science education page for session one, before the first bead leaves the table or the pipe leaves the ground. Walk through the traffic controller metaphor. Point to the reticulospinal tract language and say it plainly: the signal is too loud, not the muscle too weak. This is the page that reframes the problem from something the patient is doing wrong to something the brain is doing that we can work on. It is the foundation every subsequent session builds on.
"Understanding Muscle Stiffness, Jerks, and Fatigue" — pull this page when the patient starts noticing that their arm behaves differently in different environments — louder rooms, brighter lights, more chaotic sessions. This is not the first-session page. It is the page for the patient who says "I don't understand why it was better at home." That statement is your cue. Pull this page, point to the reticulospinal filtering explanation, and name what is happening before the patient concludes that their progress isn't real.
"Ways to Decrease Tightness" — this is the between-session strategy table. After the first session where you have established a tonal threshold and the patient has felt the difference between the arm before and after the bilateral phase, give them this page. Ask them to pick two or three strategies they can use at home — not all of them, two or three that map to their life. Write their choices on the page. A strategy table with personalized choices circled is a home program. A strategy table without them is a reference document.
"Upper Limb Recovery Strategies" — pull this page when you are transitioning the patient from the pipe to a functional object, or when they ask why the activity is changing. This is the page that explains why task-specific practice matters, why you are choosing personally meaningful objects, and why partial use still counts. It is also the page for the family member or caregiver who asks what they can be doing at home to support recovery. The "encourage regular use of the affected arm" entry is a carryover conversation starter, not just a bullet point.
"Key Milestones in Upper Limb Spasticity Recovery" — this is your progress map page, and it is most useful when the patient is demoralized. The milestone sequence — strategies, breaking out of flexor synergy, sustained holding at 90 degrees, tolerating the unaffected hand working nearby — maps directly onto the arc activity progression. When the patient can hold neutral shoulder through six chips on the arc, that is milestone 3 being built in real time. Name it as such. Patients who can see their clinical work on a progress map move differently in the session than patients who feel like they are doing the same thing over and over.
"Associated Reactions" — pull this page when the patient first notices their affected arm moving when they are working with the unaffected side. This will happen during the bilateral phase or during the transition to Level 4 and 5 of the arc when the cup demands real effort. Do not wait for the patient to be alarmed by it. If you know it is coming — and with this population you do — introduce this page proactively, one session before the level where you expect it to emerge. A patient who already understands what associated reactions are can observe them with curiosity instead of fear.
Clinical tip: Keep all six pages in a folder you bring to the session. Do not carry the full packet in to hand over at once. The patient receives the right page at the right moment — which means you have already decided before they sit down which page this session needs. That decision belongs in your session prep, not in the moment.
Stroke Upper Body Patient Resource
Handout 2: Arc Progression Resource: Clinician Reference
This is your session-side prescription tool. It does not replace your clinical judgment — it structures it. Before the patient sits down, you have already made four decisions: which level you are working at, which variable is active this session, what you are watching for, and what "stable" looks like before you advance. This reference holds all four decisions in one place so you are not making them during the session while also watching the shoulder.
Best used for: Active tracking during the session and documentation immediately after. The Watch For column is your observation guide while the task is running. The Advance When column is your end-of-session decision tool. The Documentation Language column is what you fill in before you close the note.
Clinical tip: The most important column during the session is not the documentation language column. It is the Watch For column. Read it before the patient picks up the object. Not after something goes wrong — before the first movement. Your observation is sharpest when you know exactly what you are looking for.
A clinician who is watching for "shoulder internal rotation at high chips" sees something different than a clinician who is watching the activity generally. The reference is useless if it lives in the folder. It belongs on the table.
The regression note at the bottom of the reference is not optional reading. It is the clinical reframe that prevents misinterpretation of a normal finding as a setback. Every time the object changes, read it. If you do not read it, you will read the threshold regression as failure. If you do read it, you will document it correctly — as a recalibration demand, not a plateau.
Clinical Application Guide: Running the Session with Both Handouts
Before the session — identify the target pattern and establish the patient's functional destination
Before the session — decide your level and your page
Pull the Arc Progression Reference. Identify which level the patient is at and confirm that the variable being introduced this session is the only variable changing. If you advanced the arc width last session, the object does not change today. If you are introducing the cup for the first time, the arc configuration is identical to last session. Write the level and active variable at the top of your tracking sheet before the patient arrives.
Decide which page from the Patient Resource, if any, belongs in this session. This is a one-sentence decision: "Is there something happening with this patient right now that a specific page would address?" If yes, pull the page. If no, skip it. Do not hand a page over simply because it is the next one in order.
During the session — use the Watch For column, not your general impression
The Watch For column is your observation protocol. Run the bilateral phase first and document its quality before starting the unilateral arc. The bilateral quality predicts the unilateral threshold — that relationship belongs in your note, and you can only document it if you tracked it.
When the breakdown chip appears, do not wait until the end of the arc to name it. Name it in the moment: "There — do you feel that pull? That is the signal we are working on. Can you bring the shoulder back to neutral?" Then document whether the correction held, and for how many chips. That is your motor learning data. A correction that holds for three chips and then drifts again is different from a correction that collapses immediately — both belong in the note, and they point to different intervention targets.
After the session — assign one task and connect it to the right page
Do not end the session without a between-session task. If the patient has the "Ways to Decrease Tightness" page, ask which two strategies they are using between sessions and whether those strategies are happening. If they are not, that is a dosage variable — document it. More repetitions of tonal inhibition between sessions accelerates motor learning. Absence of between-session practice is a clinical finding, not a motivational one.
If you pulled the "Key Milestones" page this session, ask the patient where they see themselves on the map. The answer tells you whether their self-assessment matches your clinical data — and whether the gap between those two is a target for your next session's education.
Tracking progress across sessions — connect the resources explicitly
Use the Arc Progression Reference to track which level the patient is at, which variable moved, and what the tonal threshold was. Use the Patient Resource to track which pages have been introduced and which between-session strategies are active.
When the patient self-reports that something is easier — when holding the plate feels more automatic, when the arm does not pull as hard when the unaffected side is working — name it, date it, and connect it to the arc level and tonal threshold data from the Reference. That connection is your functional outcome. It is also your discharge planning data. A patient whose self-report of functional improvement correlates with measurable expansion of the tonal inhibition threshold across six sessions is a patient whose discharge is supported by two converging data streams. Document both.
One-Line Clinical Reasoning Starters
- Tonal inhibition threshold identified at chip [N] of [total] — below functional demands for bilateral ADL performance — skilled arc-based inhibition training required to expand the sustained neutral window under concurrent motor load.
- Threshold regression observed at object transition from pipe to plate — documented as recalibration demand, not plateau — skilled grading required to advance object complexity without reinforcing compensatory tonal patterns.
- Shoulder internal rotation drift [gradual/sudden] at chip [N] with [adequate/inadequate] self-detection — indicates [motor endurance / error monitoring] deficit — skilled real-time facilitation required beyond unsupervised repetition.
- Bilateral synchrony quality during phase one [adequate/inadequate] — predictive relationship between phase one and phase two tonal threshold documented across [N] sessions — skilled bilateral priming protocol required to prepare inhibitory baseline for unilateral task demand.
- Compensation pattern observed [wrist deviation / grip tightening / scapular elevation] at arc position [N] — persisted / resolved with verbal cuing — skilled intervention required to [identify compensation mechanism / facilitate motor plan revision / grade load to within patient's inhibitory capacity].
- Functional criteria for bilateral ADL task performance [approaching / not yet met] — arc-based inhibition training progressing through Level [N] — continued skilled intervention required to advance object load complexity toward functional simulation at Level 6.

Responses