She knows the answer before you finish the question.
Not because she is rude. Not because she is impatient. Because the part of her brain that is supposed to catch the impulse before it becomes a word is not catching it fast enough.
She interrupts at the doctor's office...not to be difficult, but because the automatic response fires before the deliberate one can intervene. She derails conversations with tangents she cannot stop herself from following. She answers the question she expected, not the one that was actually asked.
Her family calls it a personality. Her chart calls it impulsivity.
👉 Neither of those is the right clinical frame.
This is a response inhibition deficit. The brake system is not working. And it is trainable.
This is the first newsletter in the Five Executive Functions in Practice series. Each issue targets one executive function with a specific clinical activity and a complete protocol.
This one is inhibition, the foundation everything else in this series builds on.
.What the activity actually is
The tools:
🔵 Beads — ten colors: red, purple, green, blue, orange, yellow, white, black, pink, brown
🥣 One bowl
📋 The Recipe Card — 10 steps, placed flat in front of the patient. Steps include simple counts and math operations the patient solves before placing beads. [included for members]
🃏 Recipe Rule Cards — interference cards that change the rules of the recipe mid-task [included for members]
🃏 Verbal Task Cards — interference cards requiring a verbal response, with optional clinician interruption mid-response [Included for members]
⏱️ A timer
📊 A tracking sheet: rule errors by card type, self-detected vs. clinician-identified, stop-signal success rate, recipe completion time
The setup:
The Recipe Card is placed flat on the table, visible to the patient throughout. Beads are sorted by color in front of the bowl — not mixed. The interference card stack sits face-down beside the clinician. The patient does not see the cards before they are played.
The task, in two phases:
Phase one — Recipe only. Patient works through all 10 steps without interference. This is the baseline. Time it. Count errors. Do not intervene. This is your clean single-task measure, and everything in phase two is measured against it.
Phase two — Recipe with interference cards. Patient restarts the recipe. The clinician introduces interference cards between steps or during verbal tasks. The patient must respond to the card and return to the recipe without losing their place.
👉 The recipe does not pause for the interference card. That is the point.
Before the first bead — lead with science every time
Before the recipe card goes down, say this:
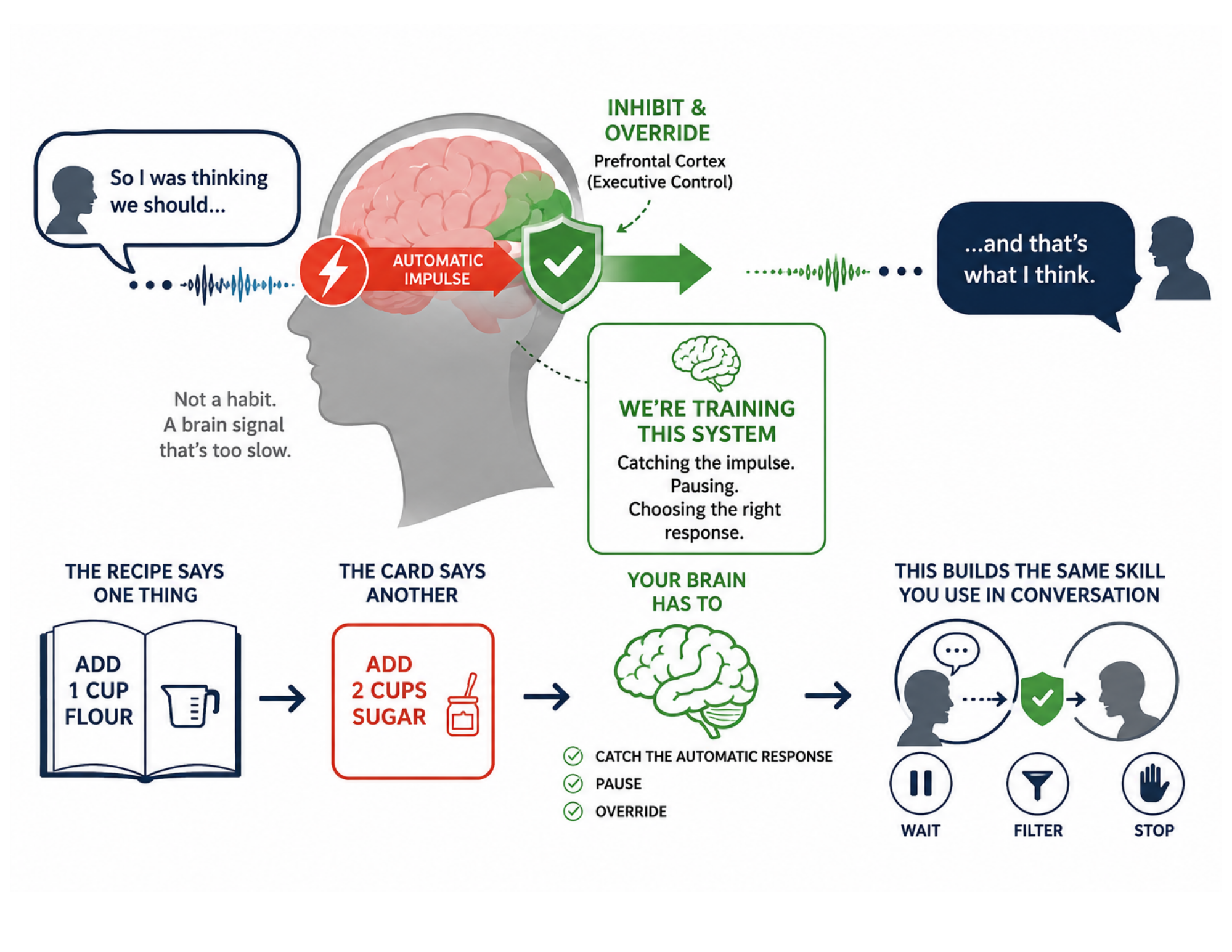
"The reason you sometimes respond before someone finishes talking (or follow a thought you know you shouldn't follow) is not a habit problem. It's a brain signal problem. The part of your brain that catches those impulses and holds them back isn't firing fast enough. What we're doing right now is training that system. Every time the recipe says one thing and the card says another, your brain has to catch the automatic response and override it. That's exactly what happens in a conversation when you need to wait, filter, or stop yourself mid-sentence."
👉 A patient who understands they are retraining their brake system practices differently than a patient who thinks they are sorting beads.
Why this is a Go/No-Go intervention
The recipe establishes the dominant response. The patient reads "3 red beads" and the automatic action is to reach for red. That pathway is fast, practiced, and efficient.
The Recipe Rule Card disrupts it. "Warm colors are no longer allowed." Now the brain has to catch the reach before it completes — identify red as a warm color, suppress the response, and select a different action. That suppression is Go/No-Go training.
👉 The dominant response has to be identified and stopped before it executes. That is the same cognitive operation required to stop a conversational tangent before it leaves the mouth.
The error you are watching for is not the wrong bead in the bowl. It is what happens in the half-second before the bead gets there.
A patient who reaches for red, catches themselves, and withdraws has an intact inhibitory system under load.
A patient who places the bead before the rule registers has a response latency problem. A patient who places the bead after appearing to read the card has an encoding problem. Three different patients. Three different intervention targets.
Why the Verbal Task Cards are a Stop-Signal intervention
The Verbal Task Cards target the second inhibition system. The patient begins generating a response like "dog, cat, bird...", and the clinician cuts in: "only nocturnal animals." The response already in motion has to stop.
That is a Stop-Signal Task. The initiated response has to be intercepted mid-execution and redirected. This is harder than suppressing a response before it starts, because the motor program is already running.
👉 This is the exact moment your patient fails in conversation. Not the moment before the interruption — the moment after it, when they cannot stop what they have already started saying.
Document whether the clinician interruption came before or after the patient began responding. A patient who fails only when interrupted mid-response but succeeds when the rule arrives before they start has a stop-signal deficit without a Go/No-Go deficit. That distinction changes the intervention.
Why the recipe is the right scaffold
A standard Go/No-Go task uses simple stimuli — a flashing circle, a color, a tap. The inhibition demand is real but the context is abstract.
The recipe makes the inhibition demand functional. The patient is managing a sequence, calculating, tracking what they have already done. The interference arrives inside that load, not beside it. That is where inhibition fails in real life. Not in quiet, structured conditions. Under cognitive load, mid-task, when the brain is already busy.
👉 The patient who passes a structured inhibition screen and fails in conversation is failing because the screen did not test inhibition under load. This activity does.

How to Treat This (Real Sessions)
🔵 Run phase one without interference every session. A clean 10-step baseline (time, error count, self-corrections) is the number everything else is measured against. If you introduce interference before you have a baseline you cannot attribute anything to anything.
👉 Count errors by type: wrong color, wrong count, wrong math. They are not the same finding. Wrong color under a rule card is an inhibition error. Wrong count on a math step is a processing error. Document which type before you decide what to address.
🃏 Introduce one card type at a time. Recipe Rule Cards first: two sessions minimum. Verbal Task Cards second. Combine both types in the same session only once the patient is stable on each type separately. Combining before that means you cannot separate which card type is driving the errors.
🧠 When the clinician interruption arrives on a Verbal Task Card, document whether it came before or after the patient started responding. This is your most important data point for separating Go/No-Go capacity from Stop-Signal capacity. Both belong in the note. They do not respond to the same intervention.
🖐️ When a rule error occurs, give the patient three seconds before intervening. If they self-detect, that is a different clinical finding than if they continue without noticing. Self-detection with self-correction is intact error monitoring. Continuation without noticing is an error monitoring deficit on top of the inhibition problem. Both belong in the note.
📊 Track four variables every session: rule errors by card type, self-detection rate, stop-signal success rate, and recipe completion time. They move independently and tell different stories.
Documentation
This is not a bead sorting activity.
Identify and document:
- Go/No-Go inhibition: dominant response suppression under recipe rule change, error latency (response initiated before rule registered vs. after), self-detection rate
- Stop-Signal inhibition: initiated verbal response intercepted mid-execution, success rate by interruption timing (pre-response vs. mid-response)
- Inhibition under cognitive load: error rate in dual-task condition (recipe + interference) vs. single-task baseline, load-dependent inhibition ceiling
👉 If you don't name it, it doesn't exist clinically.
Describe where the breakdown occurs...specifically.
Don't write "patient had difficulty with attention and impulsivity."
Write what actually happened:
- rule error on card 3 (warm colors): red beads placed before rule registered; patient self-detected after placement; did not self-correct without clinician cuing
- stop-signal failure on verbal task card 2: patient continued listing animals for 4 items after clinician interruption before redirecting to nocturnal category
- recipe completion time increased from 4:20 (baseline) to 6:45 under interference — dual-task inhibition cost of 2:25 documented
👉 Each of these is a specific, measurable, functionally meaningful clinical finding.
🧾 Tie it to function. Every note. Every session.
- conversational inhibition: suppressing automatic verbal responses mid-execution, filtering irrelevant tangents before they are spoken, redirecting when conversational rules change mid-exchange
- medical safety: processing new information mid-appointment without losing the original question or defaulting to the anticipated answer
- ADL sequencing: catching an automatic step when the sequence changes, stopping an initiated action when conditions shift
👉 This is not a bead recipe activity.
👉 This is response inhibition training (Go/No-Go and Stop-Signal systems trained simultaneously under cognitive load) with a direct, nameable line to the conversational and functional safety deficits this patient named on day one.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!

What's included:
[Resource 1] The Bead Recipe Card: your 10-step session tool with clinician answer key, ready to print and laminate.
[Resource 2] The Interference Card Table: 20 cards across two types (Recipe Rule and Verbal Task), ready to print, cut, and use immediately.