Your patient needs endurance work. Or.....that is what the referral says.
And they do. Seated balance is compromised. Upper extremity activation is weak and asymmetrical. They fatigue quickly. The goals are clear and the physical demands are real.
But here is what the referral does not say: every time your patient is working hard enough that it takes effort (i.e., every time they are at the edge of their physical capacity) their brain is also working.
The question is whether you are directing that cognitive work, or leaving it to chance.
👉 This newsletter is about choosing to direct it.
The activity in this issue uses two PVC pipes, a mat table, and a metronome. The physical demands are real. The cognitive demands are deliberate. And understanding why each layer is in the activity is what separates a conditioning drill from a multi-modal cognitive intervention.
What the activity actually is
The tools:
🔩 Two PVC pipes: one held by the clinician, one held by the patient
🎵 A metronome
📋 A tracking sheet: rule errors by transition, metronome synchrony quality, postural condition, phase of session when errors peaked
The setup:
Patient seated on a mat table without back support. Unsupported sitting is not incidental, it is the first cognitive-motor demand of the session. The postural system is already loaded before the first pipe movement begins.
The clinician sits or stands across from the patient, holding the second pipe.
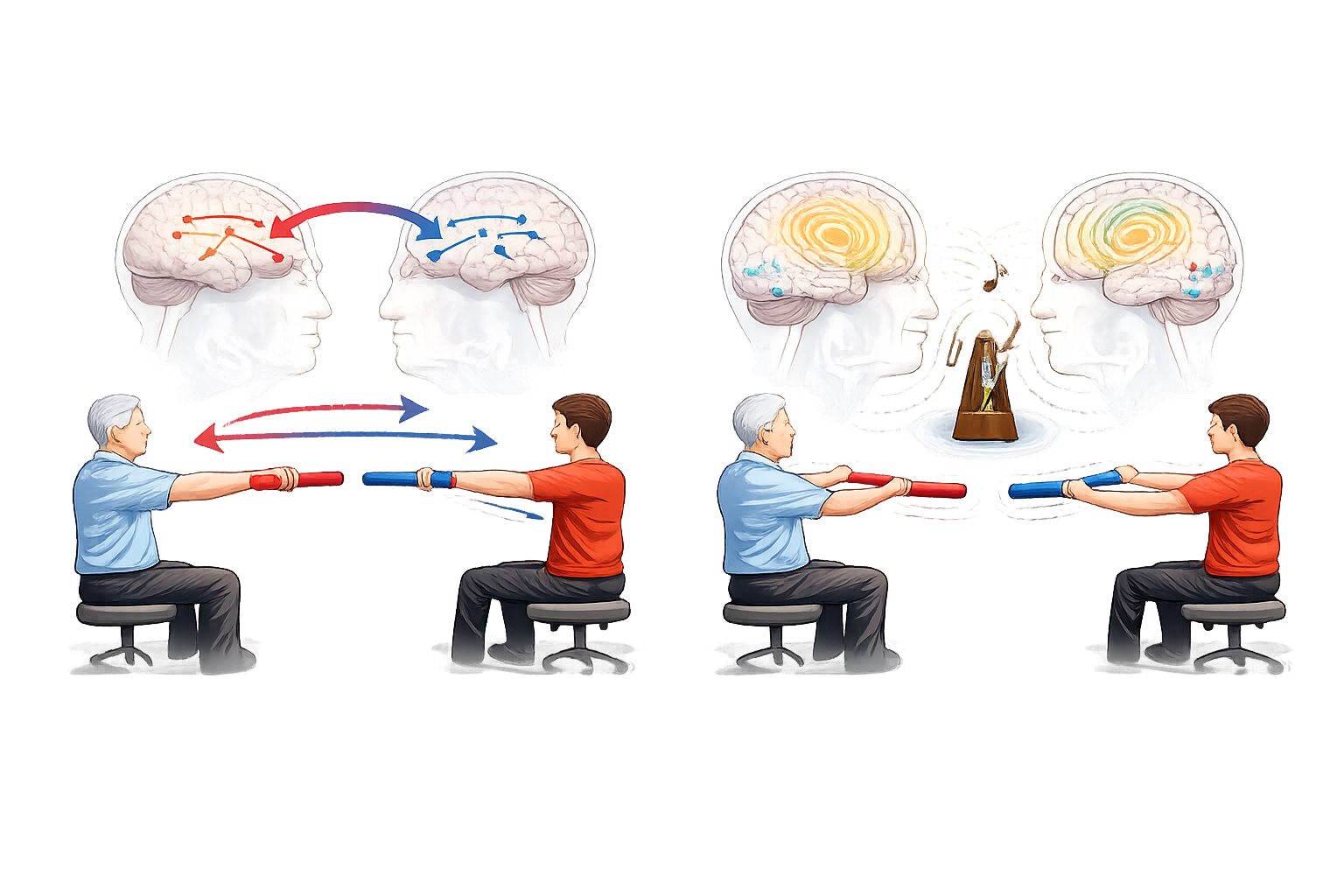
The task, in two phases:
Phase one: bilateral alternation with a contralateral rule.
The clinician moves their pipe to one side. The patient must move their pipe to the opposite side. "If I'm on this side, you use that side." That is the entire rule. It is simple to state and cognitively demanding to execute, because the natural response is to mirror the clinician, not oppose them. The patient has to hold the rule, track the clinician's position, inhibit the mirroring response, and select the correct contralateral movement...all while maintaining unsupported seated balance and bilateral upper extremity activation.
Phase two: metronome-paced sequencing.
The same alternation task is now performed to a metronome beat. The patient must synchronize movement with the external rhythm while continuing to apply the contralateral rule.
👉 That is not a timing add-on. That is a separate cognitive layer targeting a different brain region entirely.
Before the first movement — lead with science every time
Your patient thinks they are doing arm exercises. That is not what they are doing.
Before the first pipe movement, say this:
"What we're doing right now requires your brain to work in three ways at the same time. Your body has to stay balanced without support. Your arms have to move in a specific pattern. And in a minute, we're going to add a beat, which brings in a completely different part of your brain that controls timing and coordination. Every layer we add has a specific target."
👉 A patient who understands the architecture practices differently than a patient who thinks they are doing endurance work with extra steps. Name what you are doing. Every session.

Why unsupported sitting is the first cognitive layer
Removing the back support does not just increase core activation. It increases the cognitive resources required to maintain posture which directly reduces the resources available for everything else in the task.
This is the dual-task cost. It is measurable. A patient who applies the contralateral rule accurately in supported sitting and fails in unsupported sitting has not become less intelligent. They have hit their cognitive-motor capacity ceiling. The postural demand is consuming the resources the rule requires.
👉 That ceiling is your baseline. Document the postural condition every session as a controlled variable, not a setup note. When you progress from supported to unsupported sitting, expect rule errors to increase. That regression is the finding.
Why the contralateral rule is a behavioral inhibition intervention
The patient's nervous system wants to mirror what it sees. Mirroring is automatic and overlearned, it is one of the fastest motor programs in the brain.
The contralateral rule requires the patient to catch that automatic response before it executes and replace it with a deliberate, rule-governed one. That is behavioral inhibition. It is controlled by the prefrontal cortex. And it is effortful every single time — there is no version of this task where the contralateral response becomes fully automatic, because the inhibition demand is structural to the rule.
👉 Watch for errors at the moment of transition, when the clinician switches sides. That is where the inhibition demand peaks.
A patient who applies the rule correctly during a sustained position but fails at the moment of switch has an intact rule-holding capacity with an inhibitory control deficit at transition.
A patient who fails randomly across all positions has a working memory problem, the rule is not staying active.
Those are different intervention targets. Document which pattern you observe.

Why the metronome is not just rhythm, it is cerebellar training
The cerebellum is responsible for the timing, coordination, and precision of movements. It does not initiate movement, it calibrates it. One of the primary ways to engage it deliberately is through external rhythmic cueing.
When the patient synchronizes movement to a metronome beat, they are training the cerebellum to use a predictable external signal to regulate movement timing. It is the same mechanism involved in any task requiring smooth, coordinated, well-timed upper extremity function.
👉 The metronome beat is the cerebellar input. The movement synchronized to it is the cerebellar output. The gap between the two is your coordination data.
Start slow. The beat should be well within the patient's movement capacity so the synchronization demand is cognitively manageable. Errors at a slow tempo are motor coordination findings. Errors that emerge only as tempo increases are processing speed findings. They are not the same. Document which condition produced the error before you change anything.

How to Treat This (Real Sessions)
🔵 Run phase one without the metronome first, every session. Your phase one baseline is the contralateral rule without rhythm — that is your clean cognitive-motor measure for this session. Adding the metronome before you have a clean phase one reading means you cannot separate rule errors from timing errors. Protect the baseline. Phase two is only as interpretable as phase one is clean.
👉 Count rule errors by transition, not by total. How many times did the clinician switch sides? How many of those produced a rule error? A patient who makes 3 errors in 10 transitions is a different clinical picture than a patient who makes 3 errors in 4 transitions. The denominator matters. Document it.
🧠 When you add the metronome, keep everything else identical. Do not change the alternation pattern, the pace of switching, or the seating condition at the same time. One variable. If rule accuracy drops when the metronome is added, that degradation is your dual-task cost data, how much cognitive overhead rhythmic synchronization adds. Track it separately from phase one rule accuracy.
⏱️ Use tempo as a progression variable, not a difficulty dial. When the patient achieves consistent synchrony at the starting tempo for two sessions, increase the tempo by a small increment and document it the same way you would document weight on a resistance exercise. A patient who synchronizes accurately at 60 BPM but not at 72 BPM has a processing speed ceiling between those two values. That ceiling is your intervention target.
🖐️ When you see rule errors — name them, but do not correct for the patient. "You went to the same side I did, what's the rule?" The patient retrieving the rule is more therapeutically valuable than the clinician restating it. If they cannot retrieve it, restate it and document that retrieval failed. Rule retrieval failure is a working memory finding. Cuing-dependent retrieval that succeeds is a different finding. Both belong in the note.
📊 Track four variables every session: rule errors by transition, metronome synchrony accuracy, postural condition, and which phase of the session errors peaked. They move independently and they tell different stories.
Documentation
Identify and document:
- behavioral inhibition: contralateral rule accuracy across transitions, error pattern (transition-specific vs. distributed), retrieval capacity with and without cueing
- cerebellar coordination: synchrony accuracy by tempo, degradation pattern as tempo increases, dual-task cost when rhythmic demand is added to rule-based alternation
- postural cognitive load: performance comparison between supported and unsupported sitting, rule error increase attributable to postural demand
👉 If you don't name it, it doesn't exist clinically.
📍 Describe where the breakdown occurs
Don't write "patient had difficulty with dual-task activity."
Write what actually happened:
- rule errors at 3 of 8 transitions in unsupported sitting; 0 of 8 in supported sitting: postural cognitive load identified as primary variable
- metronome synchrony adequate at 60 BPM; degraded at 72 BPM: processing speed ceiling identified between these tempos
- rule retrieval failed on 2 of 3 error trials without cueing; succeeded with single verbal cue on remaining trial: cuing-dependent working memory profile
👉 Each of these is a specific, measurable, functionally meaningful clinical finding.
🧾 Tie it to function. Every note. Every session.
- any task requiring rule-following while the hands are active: medication management, cooking with a sequence, following multi-step instructions during a motor task
- any task performed in unsupported sitting or standing where cognitive load degrades postural stability
- any timed or paced functional task requiring smooth upper extremity coordination and transitions
👉 This is not seated balance training with a cognitive add-on.
👉 This is multi-modal cognitive conditioning: behavioral inhibition, cerebellar coordination, and postural cognitive load, trained simultaneously, with a direct line to functional cognitive-motor performance.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!

What's included:
[Resource 1]Dual Tasking Assessments and Interventions: your baseline measurement protocol and activity library for establishing motor-only and cognitive-only performance, calculating dual-task cost, and building a graded combination task menu across your plan of care.
[Resource 2] Brain Functions by Lobe: your session-side and patient-facing anatomy reference, updated for the Functional Cognition Lab, mapping each brain region to the specific cognitive functions being targeted in this and every multi-modal activity.