
A couple of friendly reminders:
- This is not medical advice. The content of this Newsletter is informational only.
- working memory <-- Yellow highlighted text are helpful links for you to click on.
- Member only content is at the bottom of the newsletter where you will receive...
- relevent links to resources and/or printables from the BOT Google Drive. If you are a member and have not been added to the drive for content, please request access by clicking this link.
- Clinical conversation starters that take you a bit deeper than the documentation tips in this newsletter.
- If you want to learn more about the Functional Cognition Lab inside the BOT Portal, click here.
Picture This:
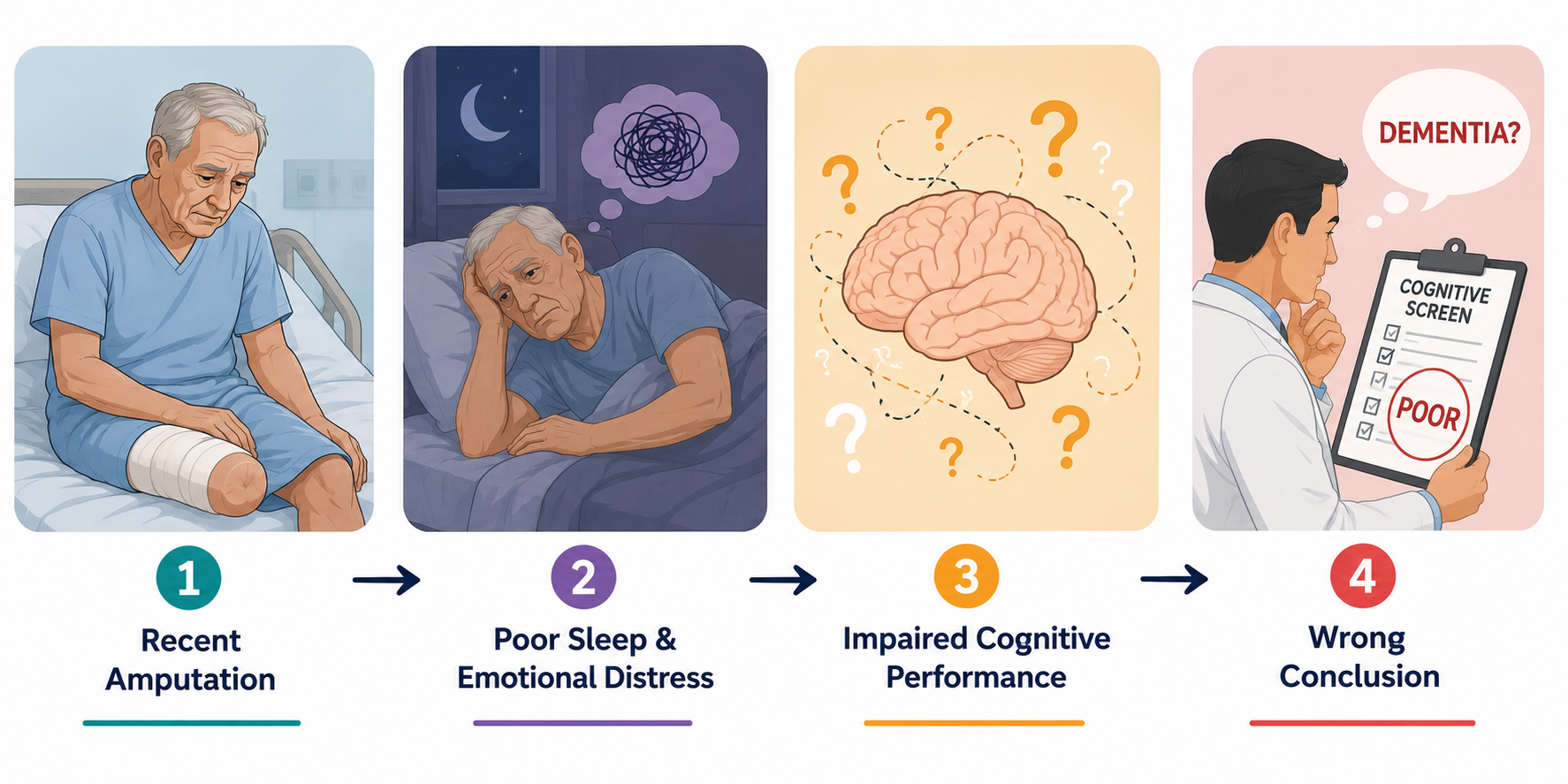
He is 76 years old. He came in for a below-knee amputation secondary to diabetic complications. He has been on the unit for four days.
His cognitive screen is poor. He cannot tell you the date. He cannot follow a three-step instruction. He loses track of what you are asking him mid-sentence.
Someone on the team has already used the word "dementia".
Nobody has screened him for depression.
Nobody has acknowledged that four days ago this man had two legs and now he has one, and that his entire understanding of his body, his independence, his identity, and his future has been catastrophically reorganized in the time it takes most people to finish a work week.
He may not be declining.
He is battling for his life on multiple fronts.
If your rehabilitation team walks into his room today focused on gait training, ADL performance, and cognitive remediation without first addressing what his nervous system is actually doing right now, you will document poor participation, low endurance, and impaired cognition and send him to a lower level of care he does not need.
This issue is about why that happens and what to do instead.
What is actually happening:
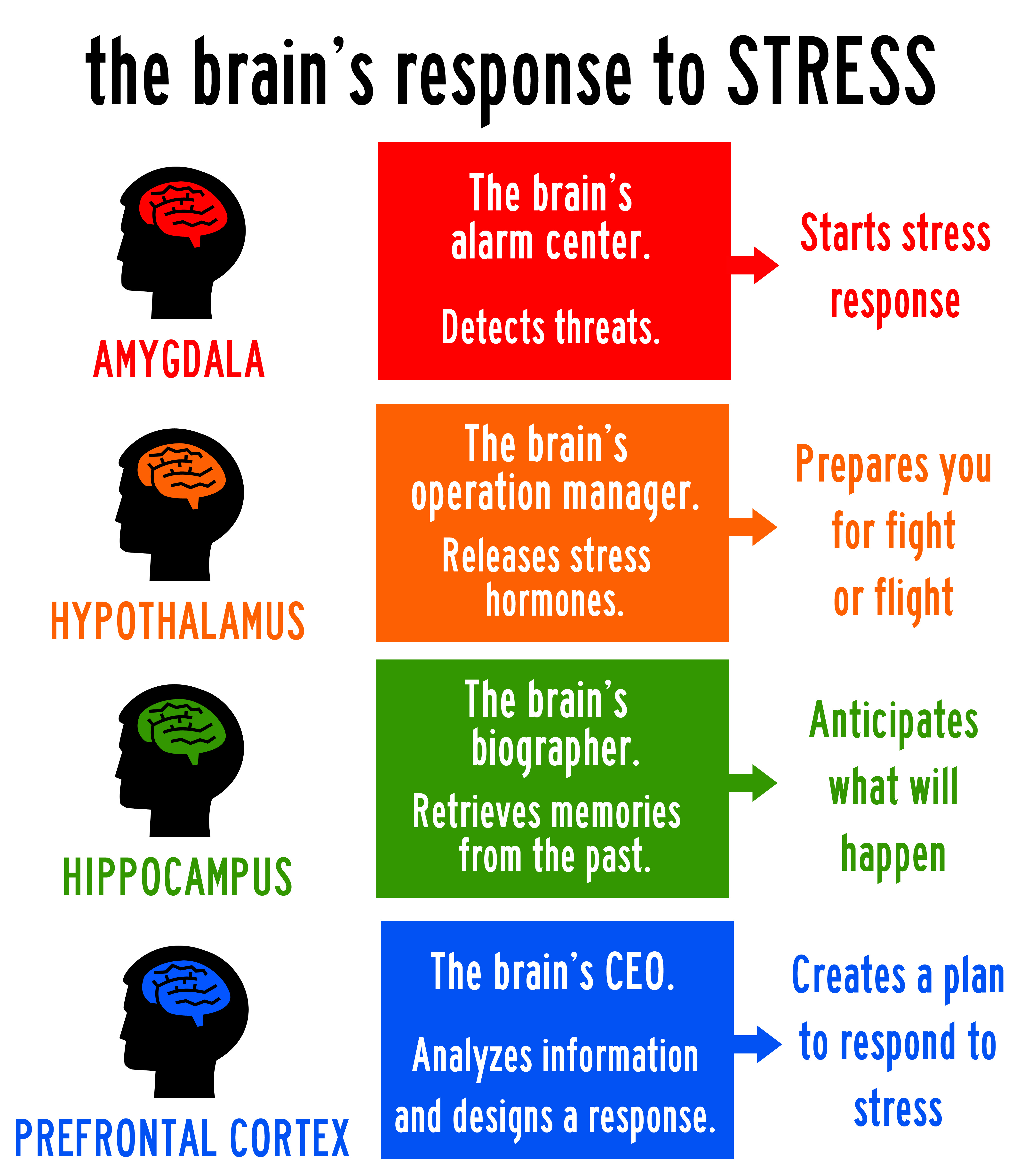
When the brain perceives threat (losing a limb is one of the most profound threats a human nervous system can register), the amygdala activates the stress response. Cortisol and adrenaline flood the system. The body shifts all available resources toward survival.
The prefrontal cortex, which governs reasoning, sequencing, working memory, and emotional regulation, goes offline.
Not permanently. Not because of dementia. Because the brain is doing exactly what it is designed to do under conditions of acute trauma.
What you are seeing on that cognitive screen is not a disease process. It may be a stress response masquerading as one.
This matters because mood-related mild cognitive impairment is real. Hospital delirium is real and it is reversible. Grief-related cognitive changes are real and they are reversible. Depression following catastrophic loss is real, it is extraordinarily common in new amputees, and it will suppress cognitive performance, physical endurance, dual-task capacity, and therapeutic participation more reliably than almost any other variable on your caseload.
And it is being missed. Systematically. Across every discipline.
His Maslow hierarchy (Maslow Patient Worksheet for Paid Member, below) has been dismantled at the most fundamental level. Safety. Body integrity. Independence. Before he can engage in rehabilitation he needs those needs to be seen, not bypassed..
Take Action
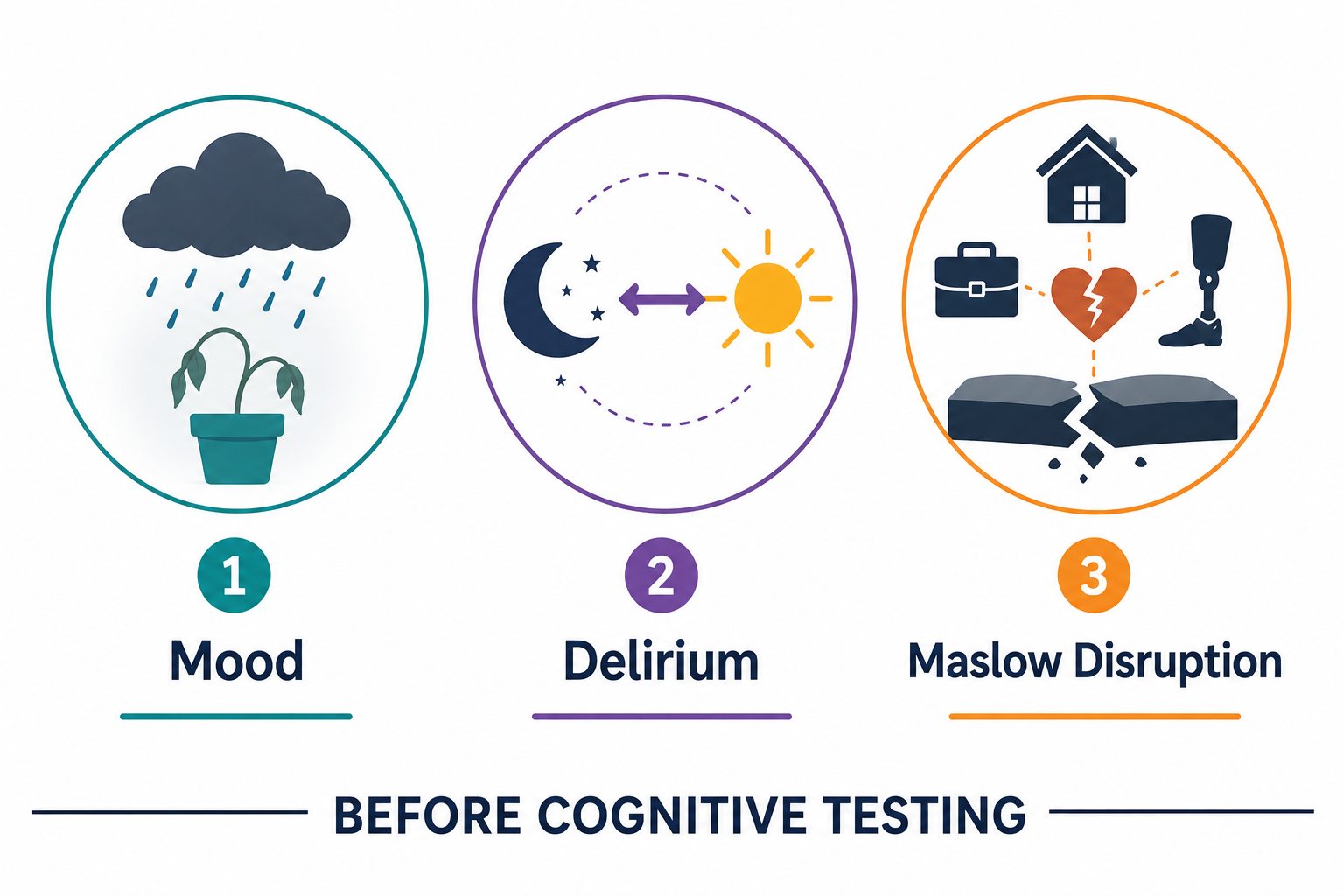
Before you begin any rehabilitation intervention with a new admission, screen for three things:
Mood.
Is this patient depressed, anxious, grieving, or in acute psychological distress? You do not need a formal tool to observe flat affect, tearfulness, withdrawal, or expressions of hopelessness. You need to look and ask, so that you can make the referral as early in the rehabilitation as possible.
Delirium.
Is the cognitive presentation acute and fluctuating, or stable and chronic?
- Delirium looks like dementia. It is not dementia.
- Fluctuating attention, disorientation that worsens at night, and acute onset following a medical event are delirium until proven otherwise.
- Speak with care people to identify new vs ongoing cognitive health.
Maslow disruption.
What has this admission cost this person? Loss of a limb. Loss of continence. Loss of home. Loss of role. A patient whose most basic needs have been disrupted cannot access the higher-order cognitive and physical capacity your intervention requires until that disruption is acknowledged and addressed.
These three screens take five minutes. They will tell you more about your patient's rehabilitation potential than any standardized cognitive assessment administered on day two of a hospitalization.
The setup:
Build this into your first contact. Before you set up your treatment space. Before you explain what you are going to work on today.
Sit down. Make eye contact. Ask one question that is not about the therapy.
How are you doing with all of this?
Then stop talking and listen to what comes back.
A patient who says fine and looks away needs more time and a safer container before they can engage. A patient who cries needs that acknowledged before any therapeutic task is introduced. A patient who expresses anger needs that anger validated before their nervous system can downregulate enough to participate.
You are not a counselor. You do not need to fix what they are feeling. You need to know what they are feeling before you decide what your session looks like today.
That is the clinical action. It is also the most underutilized intervention in rehabilitation. Be prepared to make appropriate referrals.

How to Treat This (Real Sessions)
Once you have screened for mood, delirium, and Maslow disruption, your session design changes based on what you find.
If mood is the primary barrier:
- Reduce the cognitive and physical demand of the session.
- A dysregulated nervous system has a lower endurance ceiling, a lower dual-task ceiling, and a lower frustration tolerance than a regulated one.
- This is not accommodation. This is accurate dosing. You would not prescribe the same cardiovascular load to a patient running a fever.
- Do not prescribe the same cognitive and physical load to a patient in acute psychological distress.
- Shorten the session if needed.
- Name what you are doing and why.
- Tell your patient explicitly that their brain is working harder than it looks like it is right now.
- Remind them that their nervous system is managing something enormous and that takes neurological resources away from everything else.
- This health management education is your first intervention.
- It changes how the patient understands their own performance.
- It reduces the shame spiral that compounds dysregulation.
- It builds the therapeutic alliance that makes everything else possible.
If delirium is suspected:
- Do not advance the rehabilitation program until the acute presentation stabilizes.
- Document the fluctuating cognitive profile specifically (that is, time of day, triggering conditions, duration).
- Advocate within the team for medical review of contributing factors: infection, medication, hydration, sleep disruption, pain management.
- Delirium in older adults following surgery or amputation is common and underidentified.
If Maslow disruption is the primary barrier:
Acknowledge the loss before you address the function.
A patient who has just lost a limb is not ready to learn a transfer technique until someone in the room has named what happened to them. Just asking how they are doing and what they are thinking is very important. First, it acknowledges that they are a story beyond getting them to the gym. Second, it is part of discharge planning which begins at the evaluation. You do not need to provide grief counseling, but do prioritize empathy and therapeutic use of self.
Coordinate with social work and psychology where available. Document the psychosocial barrier explicitly in your note. It justifies your modified session approach and it protects your patient from being prematurely discharged to a level of care based on a cognitive and functional performance that does not represent their actual capacity.
Across Disciplines
PT: Your patient's gait training endurance is not solely a cardiovascular or musculoskeletal finding. A patient in acute psychological distress will fatigue faster, tolerate less, and retain less from your session. Screen mood before you interpret physical performance.
SLP: Cognitive-communication performance in the acute setting is profoundly mood-sensitive. A patient who appears to have word retrieval deficits, reduced auditory comprehension, or impaired memory on bedside screening may be presenting with stress-related prefrontal suppression, not a language disorder. Rescreen after the acute mood state stabilizes before drawing diagnostic conclusions.
OT: ADL performance in the acute setting tells you what the patient can do under conditions of acute stress, unfamiliar environment, and Maslow disruption. It does not tell you what they will be able to do at home in six weeks. Document the conditions of assessment explicitly and advocate for reassessment as the acute presentation resolves.
Documentation
Identify and document:
- mood status at session onset: affect, expressed distress, engagement level, response to initial contact
- delirium indicators: fluctuating attention, disorientation, acute versus chronic cognitive presentation
- Maslow disruption: specific losses identified, psychosocial barriers to participation, referrals made
- session modification: how the treatment plan was adjusted based on mood and cognitive status and why
- performance ceiling: that today's functional and cognitive performance reflects acute mood and stress state, not baseline capacity
Do not write: patient demonstrated poor participation and limited tolerance for rehabilitation activities.
Write what actually happened:
- Patient presented with flat affect, tearfulness, and expressed hopelessness at session onset following below-knee amputation four days prior.
- Cognitive screen results consistent with acute stress-related prefrontal suppression and possible delirium, MD/Nursing staff notified.
- Presentation fluctuating across day per nursing report. Maslow disruption significant: loss of limb, independence, and occupational role identified as primary psychosocial barriers to rehabilitation engagement.
- Session modified to reduce cognitive and physical demand
- Psychoeducation provided regarding mood-cognition relationship and reversibility of current cognitive presentation. Social work referral (or Mental Health Counselor, Neuropsychiatrist, or Psychologist issued.
- Reassessment of cognitive and functional baseline recommended following stabilization of acute mood state. Current performance does not represent rehabilitation potential.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!
What's included:
[Resource 1] How Does Mood Impact Cognition (multi-page) - Patient-Facing Handout for Guided Patient Education on how mood and emotional changes may impact cognition and overall recovery.
[Resource 2] Are All Memory Disorders Permanent? Handout - Patient-Facing Handout of non-Alzheimer's reasons for acute Mild Cognitive Impairment.
Handout 1: How Does Mood Impact Your Cognition?
This is your patient-facing education resource for this issue. This may be used during the psychoeducation portion of your session. A patient who understands that their brain is not broken, that mood is actively suppressing cognitive performance in ways that are measurable and reversible, will engage with rehabilitation differently than one who believes they are declining.
Clinical tip: Point specifically to the mood-cognition loop diagram when you use this handout. Name which part of the loop your patient is currently in. Tell them explicitly that the loop is interruptible and that interrupting it is part of what rehabilitation does. That reframe is therapeutic before a single exercise begins.
Maslow Hierarchy of Needs Worksheet
Handout 2: Are All Memory Disorders Permanent? Hanout.
This handout is your most important tool for the patient who has been labeled (or who has labeled themselves) as having dementia based on an acute presentation. It distinguishes reversible from progressive causes of memory and cognitive change in plain language your patient and their family can understand.
Clinical tip: Use this handout in the family meeting as much as with the patient directly. Family members who understand that delirium, depression, and acute stress produce reversible cognitive changes will advocate differently for their loved one within the rehabilitation team. That advocacy changes outcomes.
One-Line Clinical Reasoning Starters
- Acute mood-related cognitive suppression documented
- prefrontal cortex function compromised secondary to psychological stress response following catastrophic loss
- current cognitive performance does not represent baseline capacity
- skilled psychoeducation and session modification indicated prior to advancing rehabilitation program.
- Delirium suspected based on fluctuating cognitive presentation, acute onset, and medical context
- progressive dementia diagnosis not supported by available clinical evidence, notified MD/Nursing for consult.
- Skilled monitoring and documentation of cognitive fluctuation indicated
- medical team consultation recommended prior to discharge planning based on cognitive status.
- Maslow disruption identified as primary barrier to rehabilitation engagement; loss of limb integrity, independence, and occupational role acknowledged;
- Session modified to address foundational safety and psychological needs before skill-based rehabilitation demands introduced.
See you in the next newsletter

Responses