A couple of friendly reminders:
- working memory <-- Yellow highlighted text are helpful links for you to click on.
- Member only content is at the bottom of the newsletter where you will receive...
- relevent links to resources and/or printables from the BOT Google Drive. If you are a member and have not been added to the drive for content, please request access by clicking this link.
- Clinical conversation starters that take you a bit deeper than the documentation tips in this newsletter.
- If you want to learn more about the Functional Cognition Lab inside the BOT Portal, click here.

She remembered the meeting.
She wrote it in her calendar. She got dressed. She drove there on time. She walked into the conference room and sat down.
And then everyone looked at her.
Because she had no documents. No handouts. No agenda reviewed. No prepared talking points. She had completed the last step of a ten-step preparation sequence, showing up. But, she did it without executing the nine steps that were supposed to come before it.
The meeting was not the plan. The meeting was the result of the plan. And the plan never happened.
👉 This is not forgetfulness. This is a planning deficit.
- This happened due to the inability to mentally project forward from a goal, identify what needs to happen before execution begins, and sequence those steps in the correct order before anything is touched.
It looks different from the sequencing failure that happens in the garden, where the patient prepares the soil, digs the holes, covers them back up, and waters the bed...and nothing grows because the seeds never went in. Or the laundry that runs a full cycle and comes out unclean because the machine was started before the detergent was added.
In all of these, the sequence felt complete while it was happening. Nothing triggered a stop. Nothing looked wrong. The error was invisible until the consequence arrived.
👉 That invisibility is the clinical target. And it requires two separate interventions.
- one for the planning failure that happens before execution begins
- and one for the sequencing failure that happens while execution is running.
This is Issue 4 of Five Executive Functions in Practice. The activity is a two-phase protocol using real-world scenarios. Both phases use the same five task scenarios. They target different systems.
What the activity actually is
The tools:
📋 Five scenario cards (included below for members)— written descriptions of real-world tasks, each with a disrupted sequence (steps missing, misplaced, or incomplete). The clinician holds these. The patient never sees all five at once.
📝 A blank planning patient activity guide and written lines (included below for members)— patient records corrected sequences and identifies missing steps in Phase 1
⏱️ A timer
📊 A tracking sheet: error detection accuracy by scenario, self-detected vs. clinician-identified errors, interruption recovery accuracy, number of steps lost post-interruption, scenario difficulty level.
The five scenarios:

🌱 The garden — Patient is given the sequence for planting a garden bed. The steps are: prepare the soil, dig the holes, cover the holes, water the bed. The seeds are missing. Nothing in the remaining sequence signals that anything went wrong.
🧺 The laundry — Patient is given the sequence: load clothes, select cycle, start the machine, transfer to dryer. The detergent step is absent. The machine runs. The error is not visible until the result appears.
📋 The meeting — Patient is given a sequence: get dressed, drive to the meeting, sit down. The preparation sequence — review the agenda, prepare documents, print handouts, confirm the time — is entirely absent. The arrival steps are correct. The planning steps do not exist.
🚪 Leaving the house — Patient is given the sequence: get dressed, pick up keys, lock the front door, get in the car. Missing: take medication, check the stove, lock the back door. The sequence feels complete. The non-visible steps were never in the plan.
💊 The prescription pickup — Patient is given the sequence: call the pharmacy, drive there Thursday, wait, pick up. Missing: confirm which pharmacy location, verify the prescription was actually called in, check that it is ready. The plan assumed steps rather than executing them.
The task, in two phases:
Phase one — Error Detection.
Patient reads the scenario sequence as written. Then, they must...
- identify what is wrong
- identify what step is missing, misplaced, or assumed rather than executed
- and correct the sequence before any execution begins.
The clinician does not confirm or deny until the patient has committed to an answer.
Phase two — Interrupted Task Paradigm.
Patient verbally walks through the corrected sequence in real time. At a point chosen by the clinician, an interruption is introduced (i.e., a question, a new piece of information, a competing demand). Patient must return to the sequence at the correct step without restarting from the beginning.
👉 Phase one tests whether the patient can see what is missing before it causes a problem.
👉 Phase two tests whether they can hold their place in a sequence when something pulls them away from it.
Before the first scenario lead with science
Before the scenario card goes down, say this:
"What we're working on today has two parts. The first is whether your brain can catch a problem in a plan before it becomes a problem in real life. The second is whether your brain can hold your place in a sequence when something interrupts it mid-way. These are two different skills. One lives before you start. The other lives while you're going. We're training both."
👉 A patient who understands they are training two distinct systems approaches the task differently than a patient who thinks they are reading instructions.
Why error detection is a planning intervention
Planning is prospective. It happens before execution begins. It requires the brain to mentally simulate the full sequence (from start to finish...like activity analysis :-) ), identify what steps are required, in what order, and whether any dependencies exist between steps.
The patient who shows up to the meeting without documents did not fail to execute. She failed to plan. The execution steps (i.e., getting dressed, driving there, sitting down) ran correctly. What never activated was the layer of the plan that existed before execution: the preparation sequence that was supposed to come first.
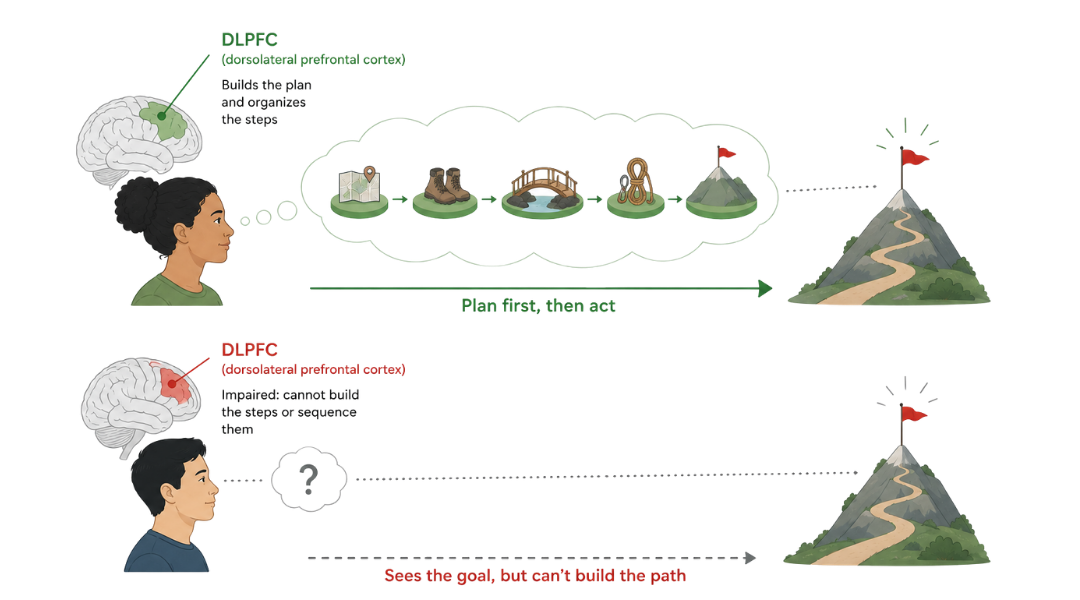
👉 The dorsolateral prefrontal cortex is the primary seat of this prospective planning function. It is responsible for maintaining a goal representation while simultaneously organizing the sub-steps required to reach it. When this system is impaired, the patient can see the goal, but cannot build the scaffolding of steps that leads to it.
The error detection task trains this directly. The patient must read a scenario, simulate the sequence mentally, identify the gap, and generate the missing step. That mental simulation is the intervention. Every corrected scenario is a repetition of the planning system being required to look forward, catch the error, and fill it in.
👉 Document whether the patient identified the missing step spontaneously or required prompting to look again. Spontaneous detection is intact prospective planning. Prompted detection is a cuing-dependent planning profile. Failure to detect even with prompting is your intervention target.
Why the interrupted task tests something different
Sequencing is concurrent. It runs during execution. It requires the brain to track position within a sequence and to know where it is, where it came from, and where it is going next...while simultaneously carrying out the current step.
When an interruption arrives, the brain must do three things: (1) process the interrupting information, (2) store the current sequence position in working memory, and (3) return to the correct step when the interruption resolves.
👉 The patient who restarts from the beginning after every interruption is not being cautious. The sequence position was lost. The working memory system that was holding their place in the sequence was displaced by the interruption, and there was no recovery mechanism.
The interrupted task paradigm trains that recovery mechanism directly. Every interruption the patient survives without restarting is a repetition of the sequence-holding system being exercised under load. Every restart is a data point = at what step did the position drop, what was the nature of the interruption, and whether the patient recognized they had restarted or believed they had resumed.
👉 A patient who restarts and knows it has a different profile than a patient who restarts and believes they are picking up where they left off. Document which you observed. They are not the same deficit, and they do not respond to the same intervention.
Why the invisible error is the clinical target
All five scenarios share a structural feature that the classic sequencing tasks do not: the error is undetectable from inside the sequence.
The patient digging the garden cannot see that the seeds are missing because everything else looks right. The patient starting the laundry cannot see that the detergent is missing because the machine is running. The patient who drove to the meeting on time cannot see that the preparation sequence was absent because arrival felt like completion.
👉 This is the clinical presentation that structured screen tools miss. A patient who passes a standard sequencing assessment in a controlled, visible environment may still fail in the real world because real-world errors are not visible. They are structural. They live in the architecture of the plan, not in the execution of it.