
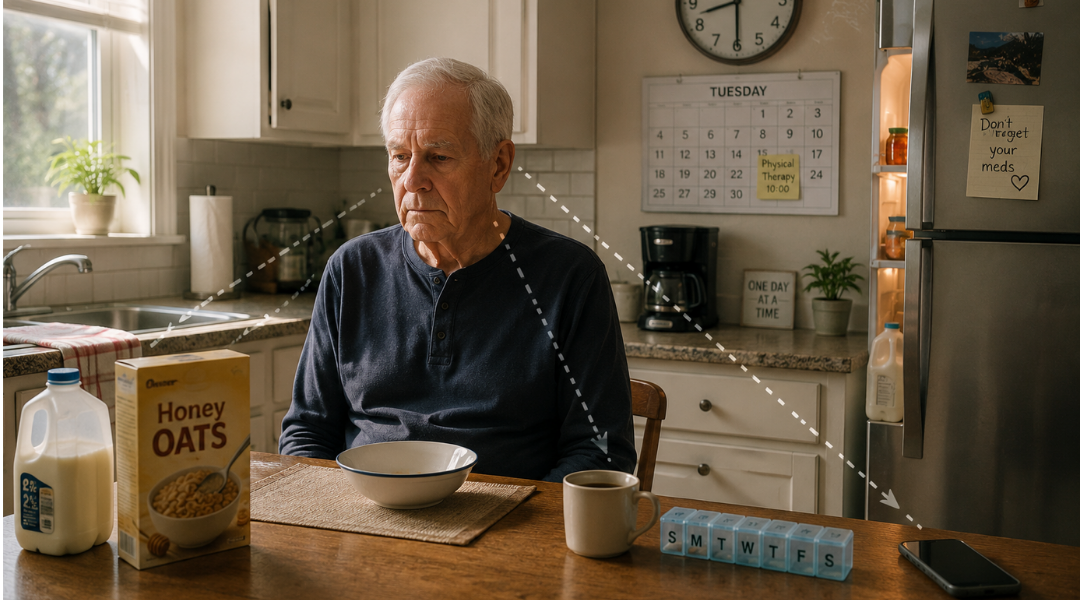
The caregiver is twenty minutes late.
This is not a crisis. The caregiver has been late before. The plan for the morning still works. The patient can wait, adjust the sequence, start with something else. There are options.
But the patient does not see the options. The moment the expected routine breaks, the cognitive system that is supposed to generate alternatives does not activate. The patient sits. Waits. Does not eat. Does not take medication. Does not call. Does not adapt.
By the time the caregiver arrives, the window for the morning routine has closed, the medication was missed, and the patient is dysregulated for the rest of the day.
This is not anxiety. This is not noncompliance. This is not a personality trait.
This is cognitive inflexibility.
Cognitive Inflexibility
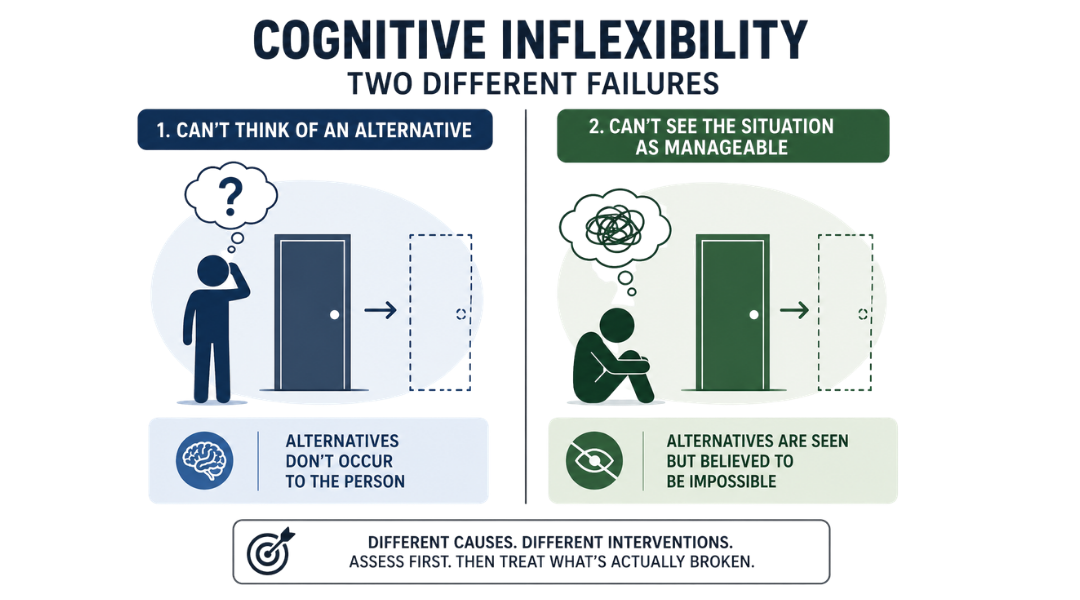
Cognitive flexibility has two distinct components that fail differently and require different interventions.
(1) The first is the inability to generate that an alternative exists.
(2) The second is the inability to perceive the situation as something that can be managed at all.
Both are present in your patient who shuts down when the furniture moves, the door is locked, or the caregiver is late.
And before you treat either one, you need to know which one is driving the presentation.

Video: Explainer video. Find on Instagram.
What the activity actually is
The tools:
🃏 One standard deck of playing cards — 52 cards, no jokers
📋 The Cognitive Flexibility Inventory (CFI) — administered at intake or first session, before the card activity begins
⏱️ A timer
📊 A tracking sheet: number of sorting rules generated in phase one, time to first alternative, phase two rule switch accuracy, number of feedback cues required before switch registered, self-generated vs. clinician-prompted switch
The setup:
Deck shuffled and placed face-down in front of the patient.
CFI score already in hand (the Alternatives subscale score and the Control subscale score).
- These two scores tell you which phase to weight more heavily this session and how to frame the task before the first card is turned over.
The task, in two phases:
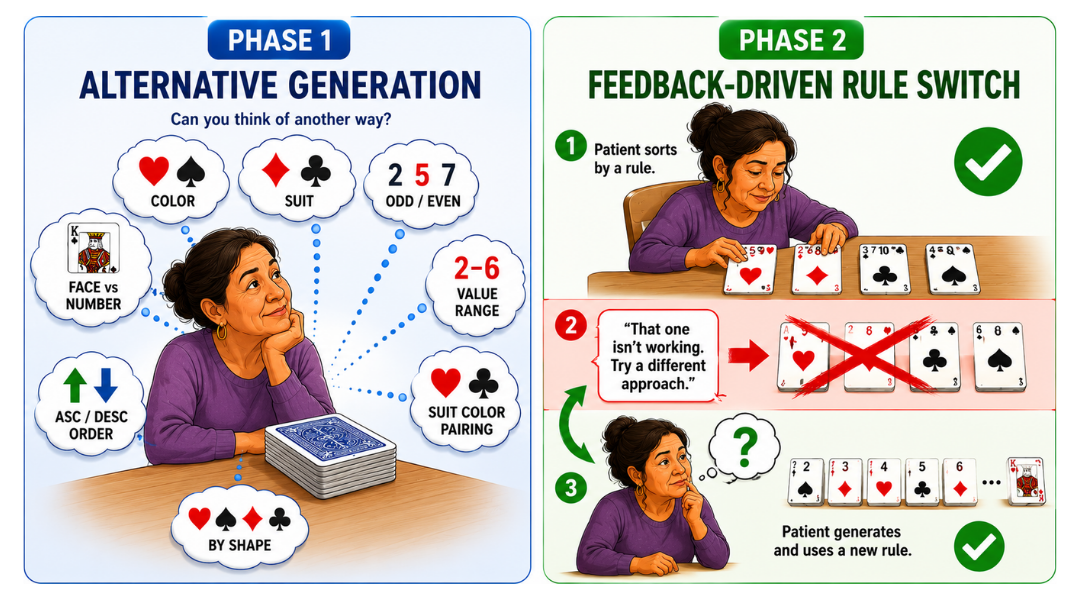
Phase one
Alternative Generation (Alternatives subscale).
Patient is asked to sort the deck as many different ways as they can think of...
- name and describe as many valid sorting rules as possible before touching the cards
- sort once by a rule of their choice.
The clinician tracks how many rules the patient generated, how long it took to reach the first alternative, and whether they stopped generating before exhausting the options.
👉 A standard deck of cards supports at least eight distinct sorting rules: color, suit, number vs. face card, odd vs. even value, value range, suit color pairing, ascending or descending order, and groupings by card shape.
So, a patient who generates one or two rules and stops is showing you the Alternatives deficit directly.
Phase two
Feedback-Driven Rule Switch (Control subscale).
Patient sorts the deck by a rule they selected. Mid-sort, the clinician says: "That one isn't working. Try a different approach." No new rule is given.
The patient must register the feedback, let go of the current strategy, infer that an alternative is required, and generate and execute one...without being told what it is.
👉 The patient whose Control subscale score is low does not fail here because they lack alternatives. They fail because the feedback feels like failure, not information. They cannot perceive the switch as something within their control. That is the target.
Before the first question, lead with science
Before the deck is touched, say this:
"When something unexpected happens at home, like when your routine is disrupted, your brain has to do two things fast. First, it has to recognize that there are other options. Second, it has to believe that those options are actually available to you. When that system isn't working well, the brain stalls. It doesn't mean you can't cope. It means we haven't trained the system yet. That's what we're doing right now. Every time you come up with a new way to sort these cards, you're training the first part. Every time you switch strategies when I tell you it isn't working, you're training the second."
👉 A patient who understands they are training two specific systems approaches the task differently than one who thinks they are playing a card game.
Why the Cognitive Flexibility Inventory comes before the activity
The CFI measures two things: (1) the ability to generate alternatives, and (2) the internal sense of control over difficult situations. They are related but distinct, and they fail independently.
A patient with a low Alternatives score but an adequate Control score knows how to manage change when they can see the options.
The problem is option blindness.
- The brain does not spontaneously generate that a different approach exists.
- Phase one is the primary intervention for this patient.
A patient with an adequate Alternatives score but a low Control score can generate options when asked but does not deploy them spontaneously because change feels unmanageable.
- The feedback-driven switch in phase two is the primary intervention
- We want to teach that feedback is information, not verdict.
👉 Both patients shut down when the caregiver is late. They shut down for different reasons. The CFI tells you which reason before you run a single card sort.
Administer the CFI at intake. Document both subscale scores. Return to them at every session. The subscale scores are your intervention targets, not the total score alone.
Why alternative generation is a trainable skill
The research on cognitive flexibility is clear: the ability to generate alternatives is not fixed.
It improves with deliberate practice.
The more times the brain is required to generate a second option after the first one is named, the more efficiently that search process runs.
The card sort trains this directly.
Every time the patient names one sorting rule and you ask "what else?", and every time they think they have exhausted the options and you tell them there are more...the brain is being required to search further than it would spontaneously.
👉 The patient who generates two sorting rules in session one and six in session four has not become more creative. They have built a more efficient alternative search pathway. That is the same pathway the brain uses when the caregiver is late and the morning routine breaks.
Document the number of rules generated every session. It is your primary Alternatives outcome variable.
Why the feedback-driven switch targets something different
Phase two does not train alternative generation. It trains something the research calls strategy-situation fit.
- The fit is the ability to recognize that the current approach is not working and that switching is both possible and appropriate.
The patient with a low Control subscale score does not fail to switch because they lack options. They fail because the moment the clinician says "that isn't working," the brain reads that as confirmation that the situation is unmanageable ...not as a cue to try something else. The feedback activates the shutdown response rather than the search response.
👉 The intervention is not giving the patient a new rule. It is giving the patient a new relationship with the feedback itself.
When the clinician says "that isn't working" and then says nothing...then waits...
That silence is the clinical moment.
The patient who sits with the discomfort and generates an alternative is learning that feedback is navigable.
The patient who looks to the clinician for the answer is showing you that the internal locus of control is not yet active.
Document which response you observed and whether it changed across sessions.

How to Treat This (Real Sessions)
🃏 Administer the CFI before the first card sort.
- The subscale profile determines which phase to weight this session. If Alternatives is the lower score, spend more time in phase one and push for more rules before allowing the sort. If Control is lower, spend more time in the phase two silence. Regardless, do not rescue the patient from the discomfort of the feedback by offering hints.
👉 Track time to first alternative separately from total number of alternatives.
- A patient who generates six rules but takes four minutes to name the first one has a different profile than a patient who generates three rules in thirty seconds.
- Latency to first alternative is your processing speed for option generation. Total count is your capacity ceiling. Both belong in the note.
🔄 In phase one, always ask "what else?" at least once after the patient stops.
- Do not accept the first stopping point as the ceiling. The patient who generates two rules spontaneously but three when prompted is showing you that the capacity exists but the spontaneous search terminates early.
🧠 In phase two, do not give the new rule. Not even as a hint.
- The moment you hint, you have taken the Control demand off the table. The patient is now executing your strategy, not generating their own. That is not phase two. Wait. If the patient remains stuck after a full minute, ask: "What do you know about the cards that you haven't used yet?" That question redirects without rescuing.
⏱️ Grade by reducing feedback specificity over time.
- Early sessions: "That isn't working, try something different." Mid-protocol: "Hmm." Late protocol: no verbal feedback. Just a neutral expression. The patient who switches on a neutral expression has internalized the cue. That is your Control subscale outcome.
📊 Track four variables every session:
- Rules generated in phase one
- time to first alternative
- number of feedback cues required before switch in phase two
- whether the switch was self-generated or required a second prompt.
They move independently and tell different stories.
Documentation
This is not a memory card game.
Identify and document:
- alternative generation: number of sorting rules generated spontaneously, time to first alternative, rules added after "what else?" prompt vs. spontaneously generated
- feedback-driven flexibility: number of clinician cues required before rule switch, self-generated vs. prompted switch, response to feedback (continued sorting, shutdown, alternative generated)
- CFI subscale profile: Alternatives score, Control score, which subscale is driving the intervention focus this session
👉 If you don't name it, it doesn't exist clinically.
📍 Describe where the breakdown occurs — specifically.
Don't write "patient had difficulty with flexibility task."
Write what actually happened:
phase one: patient generated 2 sorting rules spontaneously (color, suit); generated 2 additional rules (odd/even, value range) after "what else?" prompt; stopped at 4 total; 6 additional valid rules not identified
phase two: rule switch required 3 verbal cues before alternative was generated; switch was clinician-prompted, not self-generated; patient resumed sorting with new rule without returning to previous rule — switch held
CFI Alternatives subscale [score]: consistent with phase one performance; Control subscale [score]: above threshold — phase two difficulty attributed to option access rather than perceived controllability
👉 Each of these is a specific, measurable, functionally meaningful clinical finding.
🧾 Tie it to function. Every note. Every session.
- managing unexpected changes at home: generating alternatives when routine breaks, adapting when a strategy is not working without requiring external direction
- community navigation: identifying alternative routes, entrances, or sequences when the expected one is unavailable
- caregiver communication: switching communication or coping strategies when the current approach is not producing the expected result
👉 This is not a card game.
👉 This is cognitive flexibility training
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!
What's included:
[Resource 1] Cognitive Flexibility Inventory (CFI): your intake assessment tool establishing the Alternatives and Control subscale profile that drives intervention selection for every session.
[Resource 2] Card Sort Protocol Reference: your session-side guide mapping both phases, observation targets, grading variables, and documentation language for the full cognitive flexibility protocol.
Handout 1: Cognitive Flexibility Inventory (CFI)
Administer at intake before the first card sort. Score both subscales separately — do not rely on the total score alone. The subscale profile determines which phase to weight in every subsequent session. A patient whose Alternatives score improves while Control holds flat is a different clinical picture than one whose Control improves while Alternatives holds. Track both independently across the plan of care.
Clinical tip: The CFI is a self-report measure. Compare subscale scores to your phase one and phase two behavioral data every session. When the CFI score and the behavioral data diverge — when a patient reports high flexibility but generates two sorting rules and shuts down on feedback — the behavioral data is your clinical finding. Document the discrepancy explicitly.
Cognitive Flexibility Inventory Link
Handout 2: Card Sort Protocol Reference
Your session-side anchor for both phases. Pull it before the patient sits down. Identify which subscale is the target this session and which phase gets weighted. The grading variables for each phase are independent — advancing phase one difficulty does not require advancing phase two difficulty simultaneously.
Clinical tip: The most clinically important moment in the entire protocol is the silence after "that isn't working." Do not fill it. The length of that silence before the patient generates an alternative is your most sensitive Control subscale behavioral measure. Time it. Document it. Watch it decrease across sessions.
Visual Working Memory Grading Guide
One-Line Clinical Reasoning Starters
CFI Alternatives subscale [score]
- patient generated [N] of 8+ possible sorting rules spontaneously
- option generation deficit confirmed behaviorally; skilled alternative generation training required to expand spontaneous search beyond initial response.
Phase two rule switch required [N] clinician cues
- switch was [self-generated / clinician-prompted]
- Control subscale deficit confirmed; skilled feedback reframing required to build internal locus of control for strategy switching under unexpected conditions.
Discrepancy between self-reported CFI score and behavioral performance
- patient reports [adequate/high] flexibility; generated [N] alternatives and required [N] cues for switch
- skilled real-time facilitation required beyond self-directed practice.
Alternative generation increased from [N] to [N] rules across [X] sessions
- Alternatives subscale behavioral gain documented
- direct functional correlate for adaptive problem-solving when home routine is disrupted.
Phase two switch latency decreased from [X] seconds to [X] seconds across [X] sessions
- Control subscale behavioral gain documented
- patient increasingly perceiving feedback as navigable rather than as confirmation of unmanageability.
See you in the next newsletter


Responses