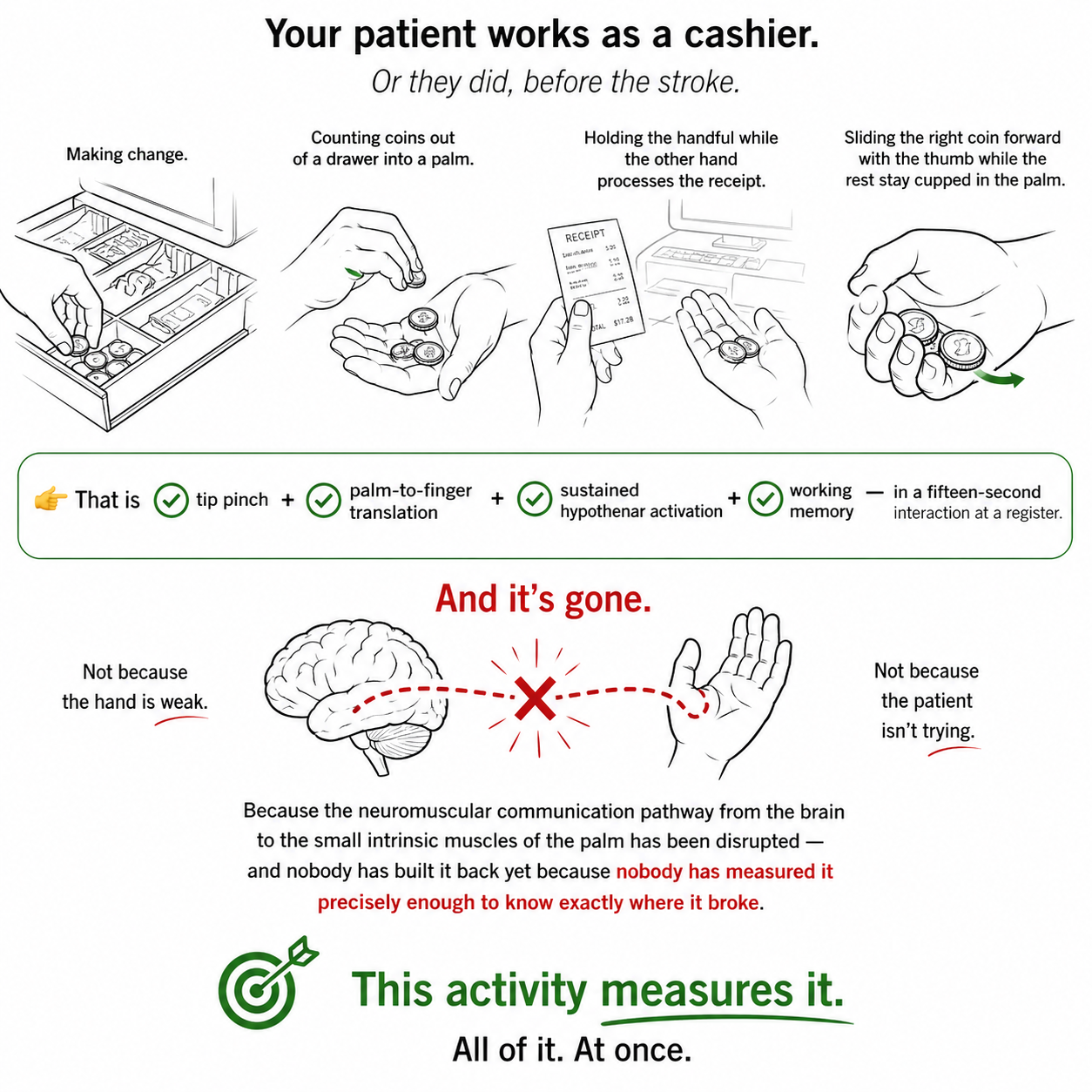
Your patient works as a cashier. Or they did, before the stroke.
Making change. Counting coins out of a drawer into a palm. Holding the handful while the other hand processes the receipt. Sliding the right coin forward with the thumb while the rest stay cupped in the palm.
👉 That is tip pinch, palm-to-finger translation, sustained hypothenar activation, and working memory...in a fifteen-second interaction at a register.
And it's gone.
Not because the hand is weak. Not because the patient isn't trying. Because the neuromuscular communication pathway from the brain to the small intrinsic muscles of the palm has been disrupted — and nobody has built it back yet because nobody has measured it precisely enough to know exactly where it broke.
This activity measures it. All of it. At once.
Fifteen beads. Five colors. PVC pipe connectors as receptacles. A timer and a tracking sheet. That is the entire setup — and it gives you endurance data, in-hand manipulation data, and working memory data in a single four-minute baseline that you can replicate at every session and track across your entire plan of care.
This is not a bead activity.
👉 This is a neuromuscular communication assessment dressed up as a bead activity.
And before the first bead leaves that palm, your patient needs to know the difference.
What the activity actually is
The tools:
🔵 15 small beads — five each of three colors, or three each of five colors
🔩 PVC pipe connectors used as receptacles — one per color, arranged on the tabletop in a consistent position before the session starts
⏱️ A timer
📋 A tracking sheet: time to complete, number of drops, number of errors, color sequencing accuracy
The setup:
Patient seated at the table with good postural alignment. All 15 beads placed into the patient's palm at once...not handed one at a time, not selected from a pile. Into the palm. Hand closes. That moment of closure is already data.
Receptacles are arranged by color directly in front of the patient, visible and within reach, not moved again until the session ends.
The task:
Patient inches each bead from palm to tip pinch, one at a time, and releases it into the correct color receptacle — while keeping the remaining beads cupped in the palm throughout.
That is one sequence. Fifteen repetitions. Every bead is a data point.
Before the first bead moves — lead with science every time
The thirty seconds before the activity begins are not setup time. They are your first clinical intervention.
If your patient thinks they are sorting beads into containers, they are sorting beads into containers. If your patient knows they are retraining the neuromuscular communication pathway between their prefrontal cortex and the intrinsic muscles of their palm, that the brain's ability to send precise, sustained signals to the small muscles that keep the hand cupped has been disrupted, and that every translation cycle in this activity is a repetition of that signal, they are doing something with a functional destination.
Name that destination before the first repetition. Every session.
"You told me it's hard to manage change at the register. What's happening is that your brain isn't sending a strong enough signal to the small muscles in your palm to keep your hand cupped while your fingers are working at the same time. That's what we're addressing right now. Every time you inch a bead up to your fingertips without dropping the ones behind it, you are retraining that signal."
👉 That is not motivation. That is encoding. The brain learns faster when the movement has meaning attached before practice begins. This is a non-negotiable part of the protocol — not a preamble to skip when the session is running long.
Patients who understand the science do not feel like they are doing kindergarten work. Patients who do not understand the science sometimes do. The science is your protection, for the therapeutic relationship and for the motor learning itself.

Why this is a sustained grasp endurance intervention
Fifteen beads in the palm. Hand closed. Pinky engaged.
👉 Watch the pinky.
The fingers doing the translation will look busy and purposeful. They are moving, they are doing something visible. The pinky is where the session actually is.
The moment the pinky begins to extend at the MCP joint, you have your finding. The hypothenar eminence is fatiguing under load. The ulnar cup is collapsing. The beads that were being contained in the palm by that ulnar border are now at risk — and your patient is about to drop one, compensate by gripping tighter with the remaining fingers, or shift into a pattern that protects the remaining beads at the cost of the translation quality.
All three of those responses are different clinical findings. Watch for which one your patient defaults to.
The thenar and hypothenar eminences together are what drive the palm's ability to cup and sustain a cup while the fingers are simultaneously active. This is not grip strength in the conventional sense. It is sustained intrinsic activation under concurrent motor demand — the palm holding while the fingers are working, both at the same time, neither able to rest while the other operates.
👉 The functional equivalent of this is every task that requires a patient to hold something in their palm while their fingers are doing something else simultaneously.
- Making change.
- Holding crackers while a child eats from your palm.
- Carrying a handful of pills to the bathroom without dropping them.
- Managing keys while unlocking a door.
- Holding a cloth while wiping a surface.
Every one of these tasks requires the same palm sustaining, fingers translating, and every one of them is inaccessible to a patient whose hypothenar eminence cannot stay engaged past the first thirty seconds of load.
Note which bead number triggered the pinky extension. Note whether it was gradual drift or a sudden drop. Note whether the patient noticed it or whether it was invisible to them. That bead number is your sustained endurance threshold. It is your baseline. That is the number you are moving across your plan of care — and it is objective, replicable, and directly functionally meaningful.
Why this is an in-hand manipulation intervention
The movement from palm to tip pinch is not a reach. It is a translation, and it is one of the most functionally demanding fine motor operations the hand performs.
The patient is not picking the bead up off a surface. They are moving it from a position inside the palm, held in place by the intrinsic muscles, upward through the digit pads to a tip pinch position at the fingertips, without using the other hand, without using a surface to assist, and without dropping the beads still remaining in the palm behind it.
Each bead is a full translation cycle:
- Intrinsic muscles shift the bead from the palm toward the distal digits
- Digits receive it and position it for tip pinch
- Tip pinch achieves the precision grip needed to release the bead accurately into the correct receptacle
- Palm re-closes. Remaining beads are re-contained.
- The cycle begins again.
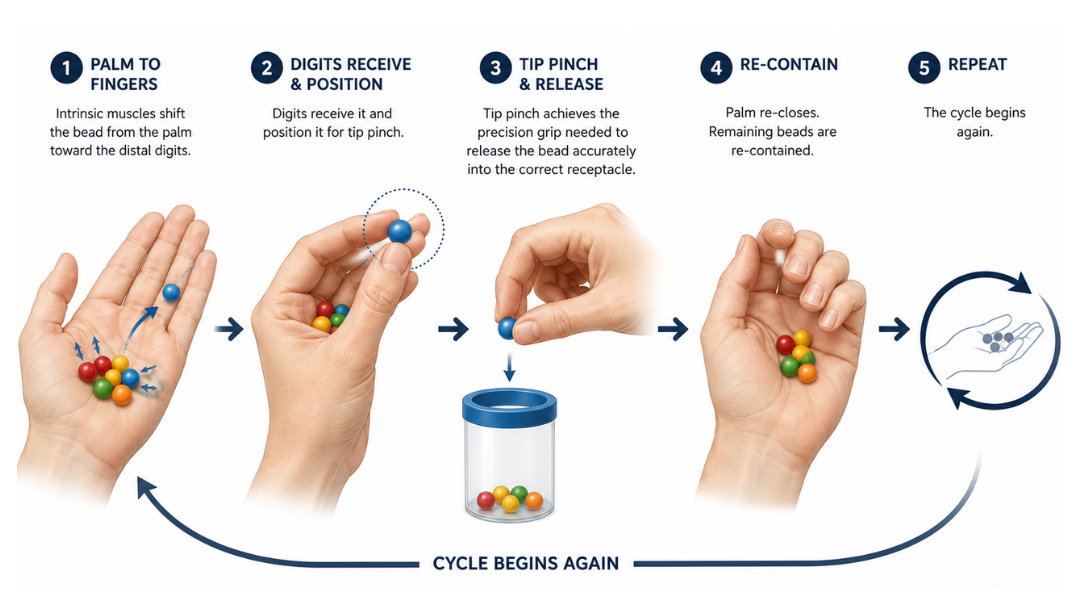
👉 Fifteen beads is fifteen full translation cycles without a break in the sustained grasp between them.
- What you are watching across those fifteen cycles is the degradation curve.
- Where does tip pinch begin to lose precision?
- Where does the patient start compensating with lateral pinch instead, sliding the bead to the side of the index finger rather than lifting it cleanly to the fingertips?
- Where does the translation slow down, or speed up at the cost of accuracy?
- Where does the release become inaccurate,dropped short of the receptacle, released too early, or pushed in rather than placed?
Each of these degradation patterns points to a different underlying impairment. A patient who maintains tip pinch accuracy but slows progressively has a motor endurance profile. A patient who maintains speed but shifts to lateral pinch compensation has a motor planning or intrinsic weakness profile. A patient who loses accuracy in the final five beads regardless of pattern has a fatigue-sensitive fine motor coordination ceiling.
👉 Document which pattern you observed. They are not interchangeable, and they do not respond to the same intervention.
Why this is a working memory intervention
Fifteen beads. Five colors. Five receptacles. A rule that must stay active for every single repetition.
Before the patient translates a bead to tip pinch...
👉 their brain has to identify the color while it is still in the palm.
Before they release it into a receptacle...
👉 their brain has to hold the color-to-location mapping while simultaneously executing the translation and the reach to the correct container.
Before the next bead cycle begins...
👉 their brain has to update the internal record of what has already been sorted without losing the spatial map of which receptacle holds which color and without letting that cognitive monitoring disrupt the motor plan for the next translation.
That is working memory. Not incidentally, structurally. The color sorting rule is a held cognitive constraint that must remain continuously active across all fifteen repetitions while the motor task runs concurrently. This is the same cognitive architecture required for medication management, for meal preparation sequencing, for any multi-step functional task where the patient must hold a rule or a plan in mind while their hands are doing something else.
👉 When the patient places the wrong color in a receptacle. That is, when they look uncertain mid-reach, pause, or glance back to check what they already sorted, that is not inattention...that is working memory failure under concurrent motor load.
Document it as such. Record how many errors occurred, at which bead number they appeared, and whether the patient self-detected the error or required external cuing to identify it.
Self-detection is a different cognitive finding than error blindness. A patient who places incorrectly and immediately notices has intact error monitoring with a working memory encoding failure.
A patient who places incorrectly and continues without noticing has an error monitoring deficit on top of the working memory load problem. Both belong in your note. Both point to different intervention targets.
The grading structure built into this task is precise and independent.
To increase the working memory demand without changing the motor demand:
- keep the same beads, same connectors, same 15-bead load
- increase the color complexity
- add a recall probe after the lids are closed
- ask the patient to retrieve a specific color by name without opening all containers.
Each variation targets working memory independently. Never advance motor and cognitive complexity in the same session.

How to Treat This (Real Sessions)
🔵 Run the first attempt without intervening. Your first trial is your baseline, not your first teaching moment. Place all 15 beads into the palm, start the timer, and let the patient work through the full sequence. Track drops, errors, and time without coaching the movement. Intervening before you have a clean baseline means every subsequent session is being compared to a number you contaminated. Protect the baseline. Everything else builds from it.
👉 Watch the pinky from the moment the hand closes. Not from the moment the first bead moves. From closure. A patient whose pinky is already drifting before the first translation cycle has a different endurance profile than one whose pinky holds through the first eight beads and then drops. Both are findings. Only one of them is visible if you start watching at bead one instead of at closure.
📐 Set the receptacles before the patient sits down and do not move them. The patient is building a spatial map of which color lives where from the moment they see the table setup. That map is the working memory scaffold for the entire task. Changing a receptacle position mid-session is not a working memory reset that makes your within-session comparison meaningless. Spatial changes belong between sessions.
🧠 Grade the working memory demand and the motor demand on completely separate tracks. If you increased bead count this session, working memory complexity stays constant. If you are introducing the delayed recall probe, the motor demand stays exactly the same as last session. One variable moves at a time. When a patient is stable at the new level across two consecutive sessions, the next variable is eligible. Treat each progression variable the way you would treat weight on a barbell.
🔄 Use the lid-covering probe as your delayed recall measure — every session once the patient is ready. After the sort is complete and the lids are closed, ask the patient to identify which color is in which container without opening them. This converts the task from a concurrent working memory demand into a delayed recall probe, a meaningfully different cognitive measure that directly parallels the functional demand of medication management, where the patient must remember what they have already taken without being able to see inside the pill organizer. Document performance on the probe separately from sorting accuracy.
📊 Track three numbers every session: time, drops, errors. They move independently and they tell different stories.
A patient whose time improves but whose drop count increases is moving faster at the cost of sustained grasp integrity. That is a motor control finding, not a strength gain.
A patient whose drop count decreases but whose error count holds steady has made a physical endurance gain without a working memory gain
These are two different intervention targets still active. All three numbers belong in the note. All three justify continued skilled care.
🖐️ When you see lateral pinch substituting for tip pinch — name it in the moment, then document it. Tell the patient exactly what you are observing and what it means: "I notice you're sliding the bead to the side of your finger instead of lifting it to the tip — that's your hand finding a workaround because tip pinch is harder right now. We're going to keep working toward the tip. Let's slow it down." Then document the compensation pattern, which bead number it appeared at, and whether verbal cuing reduced it. That cuing response is your motor learning data.
Across Disciplines (Same System, Different Look)
This is OT-led — but the cognitive and motor architecture apply everywhere.
PT: If this task is performed while seated unsupported, or while standing at a table, the sustained grasp and translation demand is now compounded by a postural cognitive load. The pinky drop threshold will be earlier. The working memory errors will increase. Document the postural condition as a controlled variable — supported sitting, unsupported sitting, standing — and track how postural demand interacts with fine motor endurance and working memory accuracy across sessions. That interaction is your dual-task postural-cognitive data.
SLP: The working memory architecture in this task — a held rule, sequential self-monitoring, and delayed recall — maps directly onto functional cognitive-communication targets including medication management, meal sequencing, and any multi-step procedure requiring the patient to track what they have already done while continuing to execute the next step. The error monitoring finding — whether the patient self-detects errors or requires external cuing — is a metacognitive measure that belongs in functional cognition documentation regardless of discipline. A patient who cannot self-monitor a color sort error under motor load is a patient whose error monitoring under communicative load warrants direct evaluation.
👉 One activity. One palm. Three disciplines worth of data.
Documentation
🧠 Document the system — not just the task.
This is not a bead sorting activity.
Identify and document:
— in-hand manipulation: palm-to-finger translation, tip pinch precision, compensation patterns observed — sustained grasp endurance: hypothenar and thenar activation under concurrent fine motor demand, pinky drop threshold by bead number — working memory: color-to-location rule maintenance across 15 repetitions under concurrent motor load, error count, error detection profile
👉 If you don't name it, it doesn't exist clinically.
📍 Describe where the breakdown occurs — specifically.
Don't write "patient had difficulty with fine motor activity."
Write what actually happened:
— pinky extension observed at bead 9 of 15 with loss of ulnar palm cup and one subsequent bead drop — tip pinch degraded to lateral pinch compensation beginning at bead 11, with two placement errors in final four beads — color sorting errors on beads 7 and 12, bead 7 self-corrected, bead 12 required clinician cuing to identify — patient unable to correctly identify more than two of five receptacle locations on delayed recall probe
👉 Each of these is a specific, measurable, functionally meaningful clinical finding.
📏 Measure the endurance threshold every session.
Document:
- bead number at which hypothenar fatigue was first observed
- total drops per session
- whether pinky drift was gradual or sudden
- whether patient self-detected the drop or was unaware
👉 An increase in pinky drop threshold across sessions is a measurable intrinsic hand endurance gain with a direct functional correlate.
Track it every session. It is your primary motor outcome variable at this stage.
⚖️ Document the dual-task cost.
When the working memory demand is active (when the patient is tracking color and location while executing translation)...
- Does motor accuracy decrease?
- Does translation slow?
- Does tip pinch precision degrade earlier than in a motor-only condition?
👉 That discrepancy between single-task and dual-task motor accuracy is your functional cognitive-motor performance ceiling.
A patient who cannot maintain tip pinch accuracy while tracking a simple color sort rule is a patient whose risk extends well beyond the clinic into medication management,
- making change,
- managing fasteners during dressing,
- any task requiring simultaneous hand control and cognitive monitoring.
Document it as a functional safety finding. Not a fine motor finding. A functional safety finding.
🔄 Capture working memory performance separately from motor performance.
Record:
- number of color sorting errors
- whether errors were self-detected or required external cuing
- delayed recall probe performance after lids are closed
- whether error rate was consistent across the sequence or concentrated in the later beads
👉 A patient whose motor performance is stable but whose working memory errors increase in the final five beads has a fatigue-sensitive working memory profile, cognitive load tolerance degrades under sustained demand.
That is a different intervention target than a patient whose errors are distributed randomly across the full sequence.
📊 Track your progression variables explicitly.
Every session, document:
- bead count used
- number of colors active
- postural condition
- whether delayed recall probe was administered
- which variable was advanced from last session and why
👉 This is cognitive-motor performance data. Treat it that way.
🧾 Tie it to function. Every note. Every session.
Make the connection explicit:
- medication management requiring sequential object tracking and small object manipulation under a held rule
- making change at a register or sorting coins
- managing small fasteners, buttons, or jewelry during dressing
- holding objects in the palm while the fingers perform a concurrent and separate task
👉 This is not a tabletop exercise.
👉 This is functional fine motor and cognitive-motor endurance training with a direct, nameable line to occupational performance.
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition
Keep Scrolling for Member-Only Content!

What's included:
- Handout 1: Why Your Pinky Matters — your patient-facing take-home resource explaining the thenar and hypothenar eminences, why the brain signal is the problem, how the bead activity connects to their real life, and what to practice between sessions
- Handout 2: In-Hand Manipulation Quick Reference — your session-side clinician reference covering all four manipulation types — translation, shift, simple rotation, and complex rotation — with mechanical definitions, functional examples, and observable compensation patterns for each
- Clinical application guide below — how to use both resources together to set up, grade, document, and progress the bead activity across your plan of care