
When someone says a patient has “memory problems,” that tells us basically nothing.
That’s like a mechanic saying your car has “car problems.”
It might sound right… but it doesn’t help you fix anything.
And in clinical practice, if you don’t know exactly what’s wrong — you end up:
- guessing
- overgeneralizing
- or defaulting to worksheets and compensation
👉 None of which actually target the problem.
Here’s the Shift
Memory is not one thing.
It is a system of systems — multiple types of memory working together, each with:
- a different job
- different brain structures
- and different treatment approaches
So when we say:
👉 “They have memory deficits”
What we should actually be asking is:
👉 Which part of memory is breaking down?
Because that answer changes everything.
🎥 Watch the Full Breakdown (22 minutes)
This walks through all 8 types of memory and how they function in real clinical practice.
-optimized_thumbnail.png) |
Think of Memory Like a 3-Story Building
To make this simple, picture memory like a building:
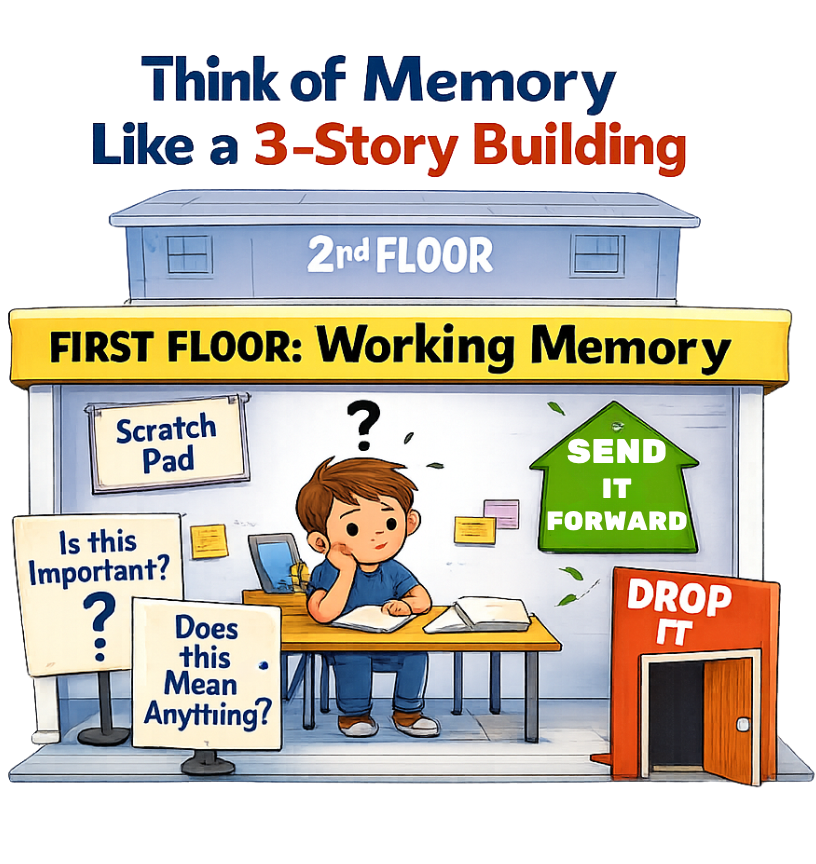
First Floor: Working Memory
This is where information first comes in.
It’s the brain’s “scratch pad” — holding information for a few seconds while the brain decides:
- Is this important?
- Does this mean anything?
If yes → it moves forward
If no → it disappears
Second Floor: Short-Term Memory
This is where information is held for:
- minutes
- hours
- sometimes a few days
This level depends heavily on the hippocampus — the brain’s memory center responsible for deciding what gets stored long-term
Third Floor: Long-Term Memory
This is the storage system.
Your patient’s:
- life experiences
- routines
- personal history
- meaningful moments
All live here.
And here’s the key:
👉 This level is often more intact than you think, even in neurological conditions.
Why This Actually Matters
If you don’t know which “floor” is breaking down, your treatment becomes too general.
For example:
- A working memory problem → patient can’t hold information long enough to use it
- A short-term memory problem → patient can’t store new information
- A long-term memory system → can often be leveraged to support learning
Same symptom on the surface.
👉 Completely different treatment underneath.
So What About the Rest of Memory?
This is where it gets interesting.
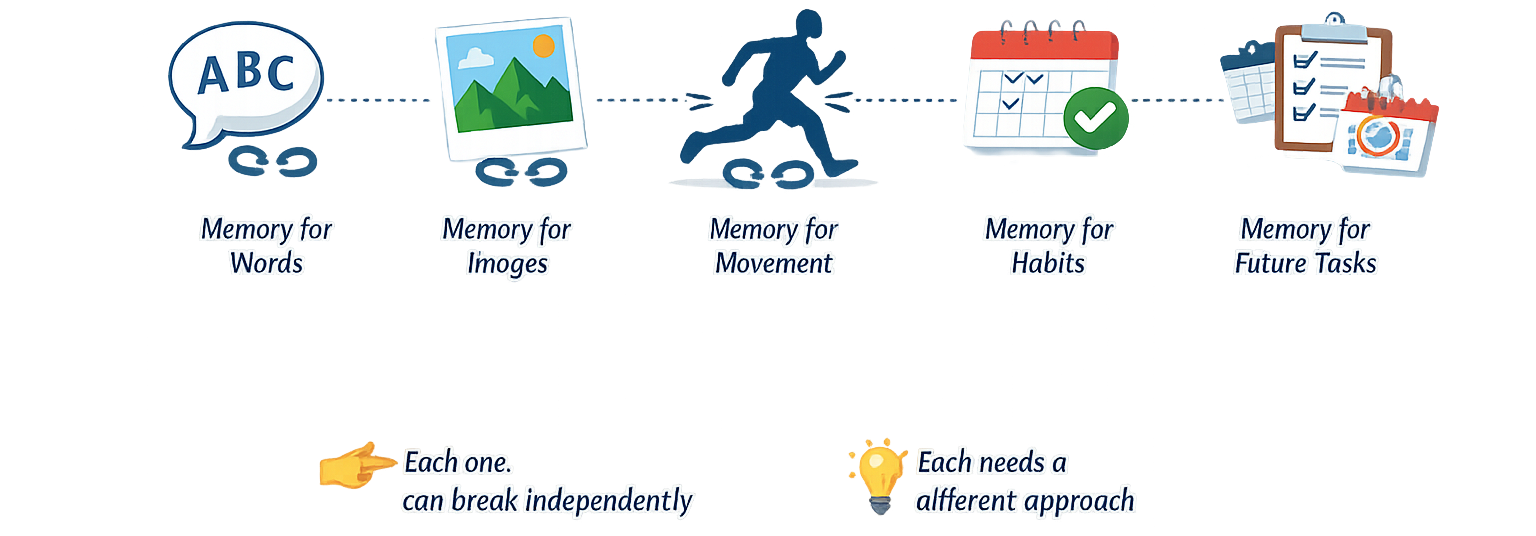
Beyond the three “floors,” there are multiple types of memory that move through this system:
- Memory for words
- Memory for images
- Memory for movement
- Memory for habits
- Memory for things you need to do in the future
Each one:
👉 can break independently
👉 and each one needs a different approach
The Clinical Problem Most People Miss
Most clinicians stop at:
👉 “memory impairment”
And jump straight to:
- calendars
- reminders
- repetition
But if you haven’t identified:
👉 which system is actually impaired
You’re not treating the root problem.
You’re working around it.
The Takeaway
“Memory problems” is not a diagnosis.
It is a starting point.
And your job is to ask:
👉 Where in the system is the breakdown happening?
Because once you know that…
👉 Treatment becomes targeted
👉 Interventions make sense
👉 And outcomes actually improve

Next Step
In the next issue, we’re going to break this down clinically:
👉 How to identify which memory system is impaired
👉 What to look for in real patients
👉 And how to stop guessing during treatment planning
Next: “Where Memory Actually Breaks (Clinically)
Author Information:
Michelle Eliason, MS, OTR/L
Occupational Therapist & Functional Cognition Educator
Owner, Buffalo Occupational Therapy
PhD Candidate, Rehabilitation Science
Founder of BOT Portal — a clinical system for real-world cognition

Responses